

Author: Marcia Correia Abreu dos Santos
Date of first publication: 16.04.2020
Last change: 20.02.2023
Changed categorization to exclude ApplicationMechanical power has become a hot topic in discussions about optimizing ventilator settings for critically ill patients.
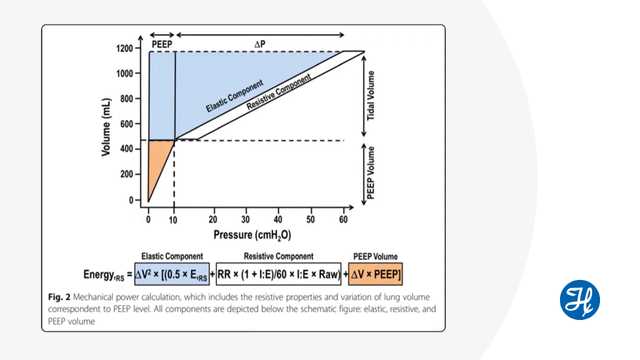
Defined as the amount of energy transferred from the ventilator to the respiratory system within a given timeframe, mechanical power has been related to the degree of ventilator-induced lung injury. In our Journal Club review, we look at what contributes to mechanical power, how to quantify it at the bedside and its relevance for applying lung-protective ventilation. The discussion in the video available below is based on the 2019 publication "Power to mechanical power to minimize ventilator-induced lung injury?".