


Estaremos encantados de ayudarle y nos pondremos en contacto con usted lo antes posible.

Nuestro equipo global y nuestros expertos locales están listos para ayudarle.

Acceda a todos los documentos, vídeos, artículos, módulos de formación en línea y recursos adicionales relacionados con todos nuestros productos.
Nuestro modo de ventilación inteligente le permitirá olvidarse de girar el pulsador para limitarse a supervisar los datos. INTELLiVENT-ASV reduce el número de interacciones manuales con el respirador (
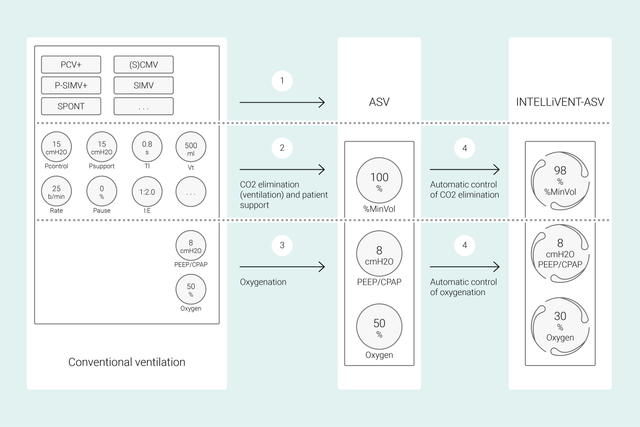
En los modos convencionales, se pueden ajustar diversos controles del respirador (como el volumen tidal o la presión, la frecuencia respiratoria, la FiO2, la PEEP y el tiempo espiratorio e inspiratorio) para lograr ciertos objetivos clínicos. Además, todos estos controles se tienen que reevaluar y reajustar con frecuencia.
Con INTELLiVENT-ASV, las estrategias y objetivos clínicos definidos para la oxigenación y la ventilación son la prioridad. Una vez definidos estos objetivos, puede decidir en qué medida tiene que controlar INTELLiVENT-ASV la oxigenación y la ventilación para alcanzar los valores deseados.
A continuación, INTELLiVENT-ASV selecciona automáticamente los ajustes del respirador, gestiona la transición entre los estados pasivo y activo, y asiste activamente en los protocolos de retirada automatizados mediante la opción Destete ráp.
Numerosos estudios internacionales han demostrado la seguridad y el rendimiento de INTELLiVENT-ASV en distintos supuestos clínicos, desde una cirugía cardíaca (


Ahorramos tiempo gracias a INTELLiVENT-ASV, que nos permite realizar otras tareas importantes de la UCI, como atender a los pacientes y proporcionar una asistencia médica imprescindible.
Enfermero de la UCI
Hospital intercomunitario, departamento de Var, Francia
El concepto de Hamilton Medical de establecer la ventilación automática en la UCI es sin duda un paso en la dirección correcta.
Jefe de la UCI
Grisons Cantonal Hospital, Chur, Suiza
Desde el punto de vista de los cuidados clínicos, INTELLIVENT-ASV nos permite realizar el trabajo que no se ve en un paciente mientras atendemos otras obligaciones más críticas relacionadas con la toma de decisiones.
Intensivista, medicina interna y servicio de urgencias desde 2018
Hospital Central Universitario de Lisboa, Lisboa, Portugal


En este vídeo, el Dr. Jean-Michel Arnal, intensivista jefe, nos ofrece una rápida demostración de las funciones y ajustes principales de INTELLiVENT-ASV con un paciente de UCI real.
En primer lugar, hay que definir la altura, el sexo y, si procede, el estado especial del paciente: SDRA, hipercapnia crónica o lesión cerebral. A continuación, debe definir los objetivos clínicos en cuanto a oxigenación (SpO2) y eliminación de CO2 (PetCO2) para su paciente.
Después, puede definir otras muchas opciones para ajustar INTELLiVENT-ASV con mayor precisión. Por ejemplo, tiene la posibilidad de determinar si desea ajustar la PEEP manualmente o si prefiere que INTELLiVENT-ASV la ajuste dentro de un intervalo que usted mismo defina. Una vez revisados o ajustados los límites de alarma, todo estará listo para comenzar la ventilación.
INTELLiVENT-ASV implementa su estrategia a pie de cama. En lugar de tener que modificar con frecuencia diversos ajustes individuales, podrá supervisar y redefinir dichos ajustes y la estrategia definida solo cuando sea necesario.
El propósito de INTELLiVENT-ASV es lograr que el paciente alcance los valores objetivo definidos y que los mantenga sin dejar de suministrar la ventilación con protección pulmonar (
Estos datos se miden a través de tres sensores: El sensor de flujo proximal proporciona datos de la mecánica pulmonar y la actividad del paciente, mientras que los sensores de SpO2 y CO2 proporcionan datos de la oxigenación y la eliminación de CO2.
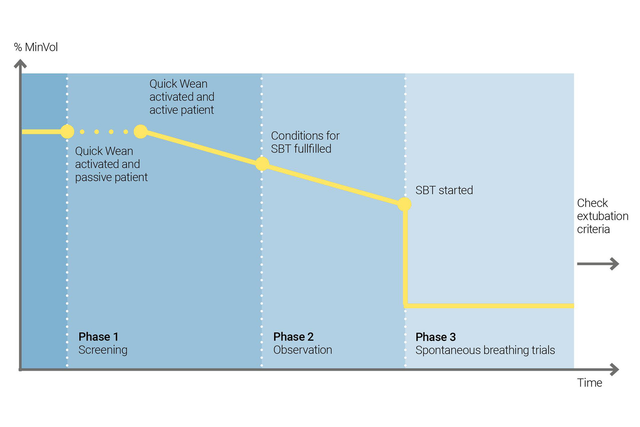
Utilice la opción de Destete ráp. de INTELLiVENT-ASV para implementar el protocolo de retirada. Puede activar esta opción durante la ventilación siempre que el paciente respire de manera espontánea.
Para configurar Destete ráp., hay que activar las SBT para evaluar si el paciente está preparado para retirarle la ventilación. solo tiene que ajustar los criterios para iniciar una SBT, definir los ajustes que se deben utilizar mientras se lleva a cabo la SBT y especificar los criterios de cancelación de la prueba.
INTELLiVENT-ASV siempre muestra el historial de todas las SBT realizadas. Si una SBT no se realiza correctamente, INTELLiVENT-ASV restablece los ajustes de ventilación anteriores.
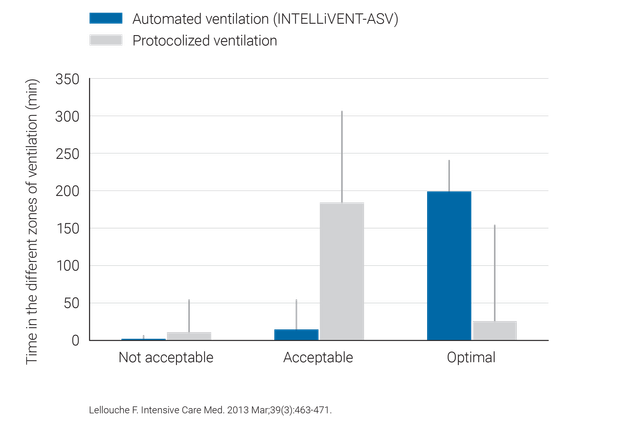
Los estudios clínicos han demostrado que INTELLiVENT-ASV es capaz de seleccionar una presión de trabajo (
INTELLiVENT-ASV requiere menos ajustes manuales que la ventilación convencional y, por tanto, alivia la carga de trabajo del equipo de sanitarios (

INTELLiVENT-ASV está disponible de forma opcional para HAMILTON-G5, HAMILTON-C6, HAMILTON-C3, HAMILTON-C1 y HAMILTON-T1, y se incluye de serie en HAMILTON-S1.



