


Nous serons ravis de vous aider et nous vous répondrons dès que possible.

Notre équipe multinationale et nos experts locaux se tiennent prêts pour vous aider.

Accédez à l'ensemble des documents, vidéos, articles, modules d'e-learning et autres ressources relatives à tous nos produits.
L'œil exercé d'un expert de la ventilation est capable de détecter des asynchronies en analysant les profils des formes d'ondes de débit et de pression.
Cependant, l'expert ne peut pas toujours être au chevet du patient et l'état du patient peut changer d'un cycle à l'autre.
C'est là qu'intervient l'IntelliSync+. Cette technologie imite l'œil de l'expert pour identifier les signes des efforts du patient (déclenchement) ou de relâchement (cyclage) sur la forme d'ondes.
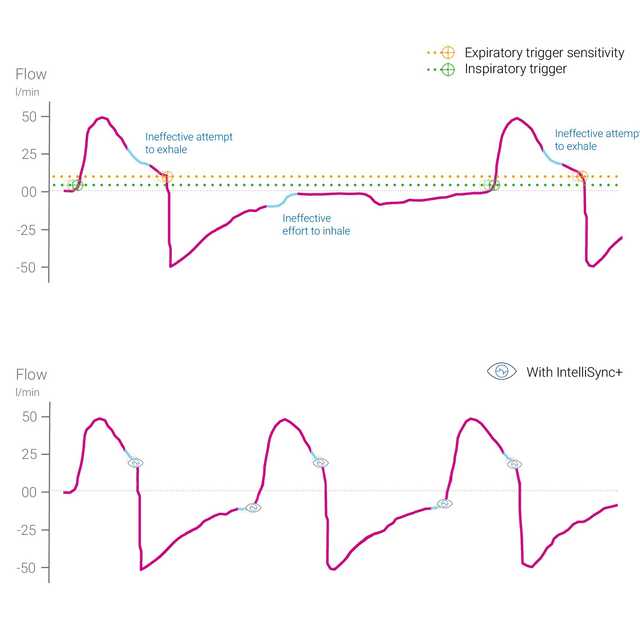
L'IntelliSync+ analyse en continu des signaux de formes d'ondes plusieurs centaines de fois par seconde. L'IntelliSync+ peut alors détecter immédiatement les efforts du patient et initier l'inspiration et l'expiration en temps réel, remplaçant ainsi les réglages de déclenchement classiques de l'inspiration et de l'expiration.
Pour une flexibilité optimale, vous pouvez choisir d'activer l'IntelliSync+ pour le déclenchement inspiratoire ou le déclenchement expiratoire, ou bien les deux.

Des asynchronies patient-ventilateur importantes sont détectées chez environ 25 % de l'ensemble des patients ventilés mécaniquement (
L'analyse des formes d'ondes est une méthode fiable, précise et reproductible permettant d'évaluer l'interaction entre le patient et le ventilateur. L'automatisation de cette méthode peut permettre un monitorage continu des patients ventilés et/ou améliorer le déclenchement des cycles et le cyclage (
Mojoli F, Orlando A, Bianchi IM, et al.
Une étude récente a montré que la commande automatisée du cyclage d’un ventilateur basé sur l’analyse en temps réel des formes d’ondes fournissait un moyen fiable d’améliorer la synchronisation chez les patients ventilés mécaniquement.


L'IntelliSync+ est une méthode totalement non invasive qui ne nécessite ni matériel ni accessoire supplémentaire. Il vous suffit d'activer l'option sur votre ventilateur pour l'utiliser en mode de ventilation invasive ou non invasive sur des patients adultes et enfants.
Comme l'IntelliSync+ peut également être combiné avec des déclenchements classiques, vous pouvez choisir de l'utiliser pendant l'inspiration, l'expiration, ou les deux.

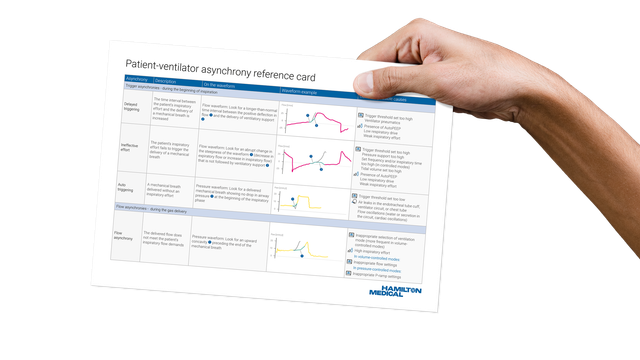
Notre carte de référence des asynchronies fournit un aperçu des types d'asynchronies les plus courantes, leurs causes et comment les détecter.
L'IntelliSync+ est disponible en option sur le HAMILTON-C6 et le HAMILTON-G5, et comme fonctionnalité standard sur le HAMILTON-S1.
