


Author: Munir Karjaghali
Date of first publication: 18.02.2019
Ventilation is effective when it removes CO2 at a rate that maintains a normal or a targeted pH.
PaCO2 is the partial pressure of CO2 in the arterial blood and represents the balance between CO2 production and elimination (V’CO2). The minute ventilation (V’E) is the total volume moving in or out of the lungs per minute, and includes the portion of tidal volume (VT) that enters the dead space of the lungs (dead space ventilation) and is exhaled unchanged. The alveolar ventilation (V’alv) is the volume that actually reaches the alveoli and actively participates in the gas exchange.
So PaCO2 is directly related to the rate of CO2 production and elimination, and inversely related to the alveolar ventilation.
PaCO2 α V’CO2/V’alv
PaCO2 α V’CO2/(V’E-V’D)
From these two equations we can see that if V’alv decreases, PaCO2 will rise - unless there is a compensatory increase in minute ventilation (V’E).
How can we achieve effective ventilation by using volumetric capnography?
When implementing a low VT strategy in patients, assuming the patient’s metabolic rate is not changing (steady V’CO2), you can use bedside measurements of V’alv and volumetric capnography to calculate the increase in respiratory rate needed to maintain or reach the desired level of PaCO2. In order to maintain the same level of V’alv and thus keep PaCO2 constant, this means there must be a compensatory increase in V’E when implementing low VT ventilation.
The optional volumetric capnography function on Hamilton Medical ventilators (
Determine the value of V’alv that helped to maintain or reach the desired level of PaCO2.
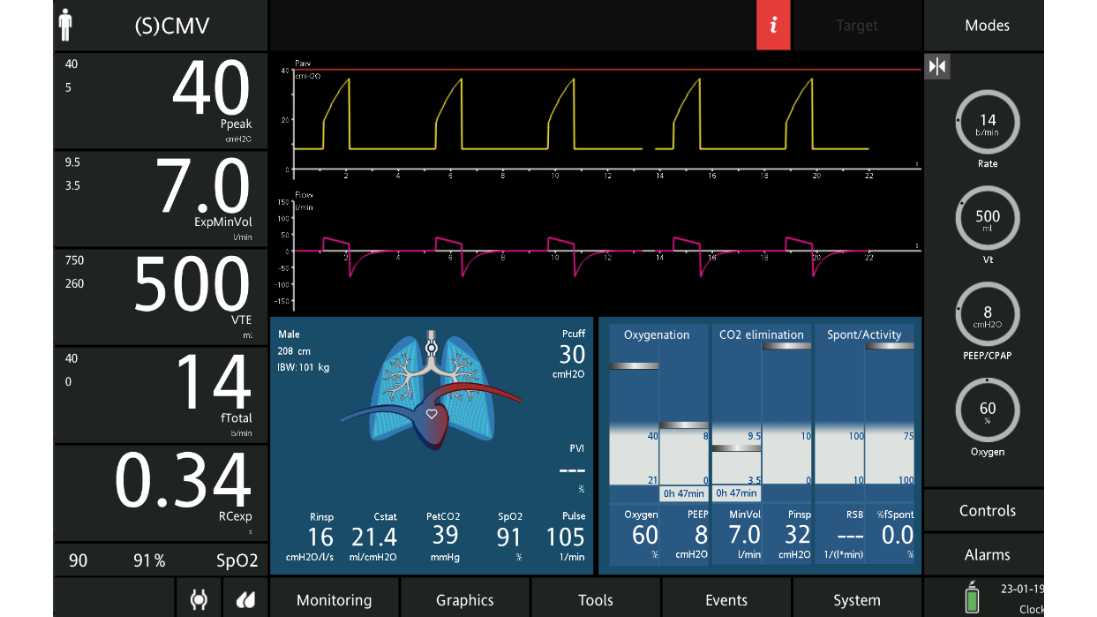
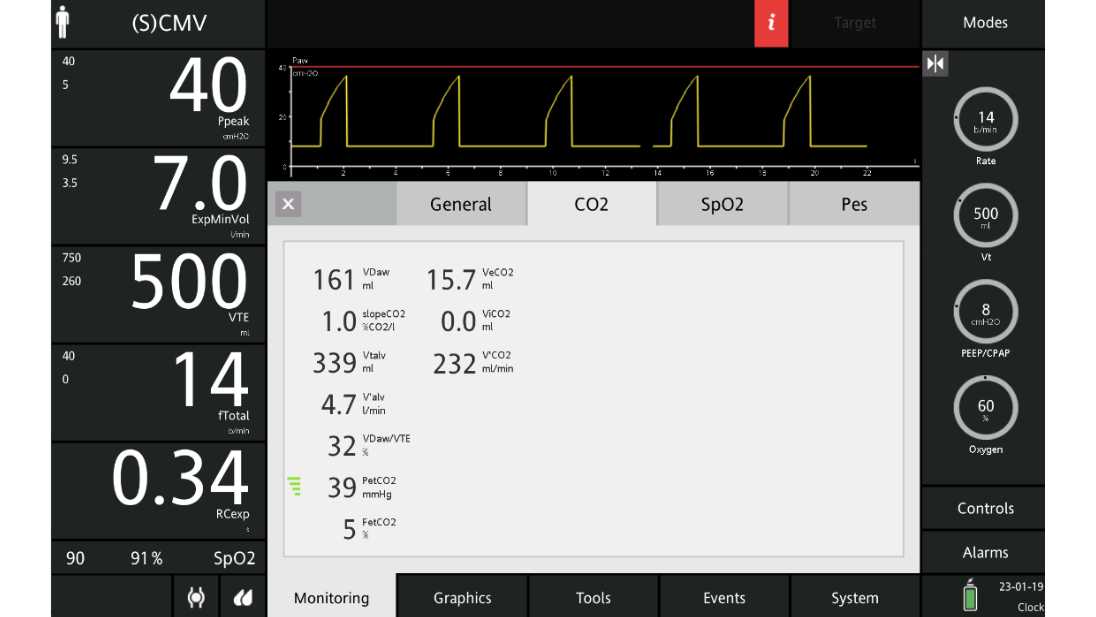
This patient, for example, was receiving volume-controlled breaths with a set VT of 500 ml at a rate of 14 b/min, an inspired fractional oxygen concentration of 0.60, and positive end expiratory pressure (PEEP) of 8 cmH2O. Arterial blood gas measurements obtained shortly after arrival were: pH 7.36, PaCO2 40 mmHg, and PaO2 65 mmHg. PetCO2 at that time was 39 mmHg. The patient’s calculated ideal body weight was 70 kg, Ppeak was 40 cmH2O, V’E was 7 l/min, and V’alv was 4.7 l/min as shown in Figures 1 and 2 below.
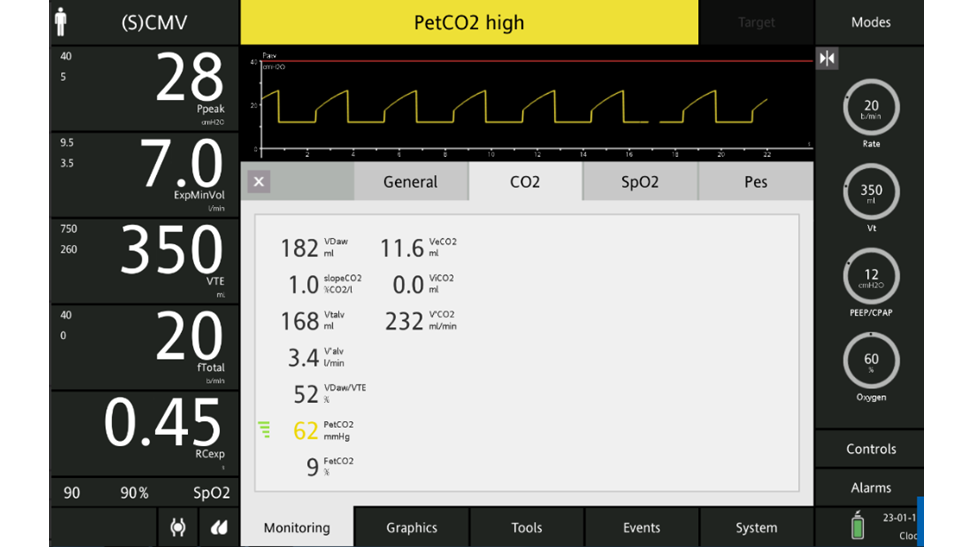
Based on a goal of 6 ml/kg ideal body weight, the VT was reduced to 350 ml, and the set respiratory rate was increased from 14 b/min to 20 b/min to maintain the same V’E (7 l/min).The decrease in tidal volume was accompanied by a drop in peak pressure to 28 cmH2O and plateau pressure to 24 cmH2O. After ten minutes, arterial blood gas measurements showed a pH of 7.17, PaCO2 of 70 mmHg, and PaO2 of 68 mmHg. Although the increase in respiratory rate was sufficient to keep V’E constant (7 l/min), V’alv fell by almost 30% (4.7 l/min to 3.4 l/min) due to an identical increase in dead space ventilation. PaCO2 and PetCO2 increased accordingly (see Figure 3 above).



Increase the respiratory rate to achieve the targeted V’alv that helped to maintain or reach the desired level of PaCO2.
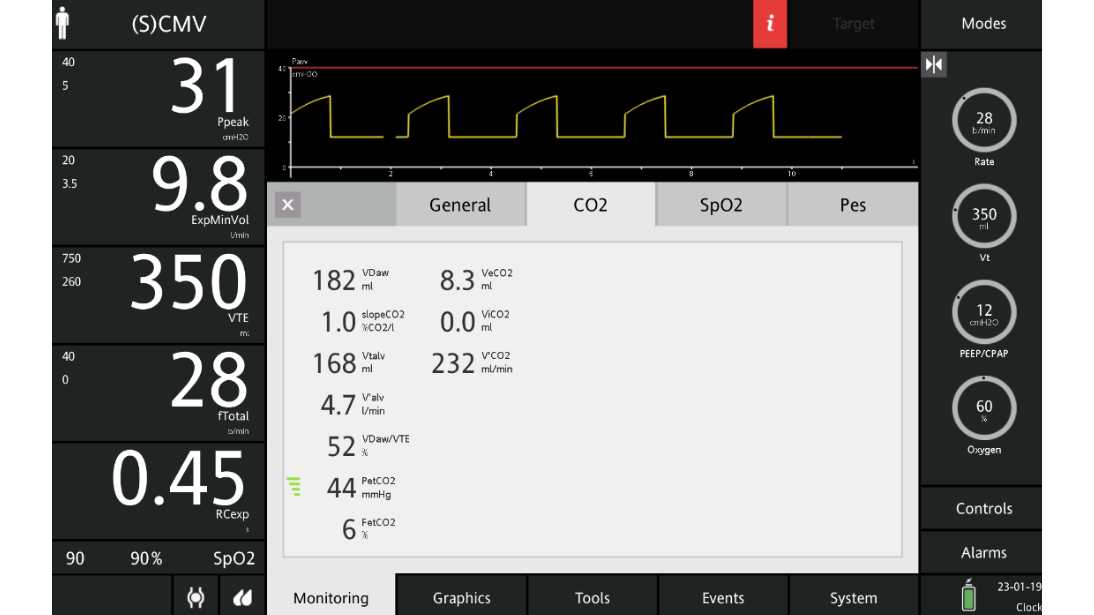
In order to achieve effective ventilation and wash out the CO2 to maintain a normal pH, the respiratory rate was increased to 28 b/min to increase V’alv to the prior level (4.7 l/min). At V’alv of 4.7 l/min, PetCO2 decreased to 44 mmHg and PaCO2 to 46 mmHg (see Figure 4 above).
The table below shows the effect of changes in VT and respiratory rate on V'CO2, V’E, V’alv, and PetCO2.
Full citation see below (
|
RR VT (ml) |
14 |
20 |
28 |
|
VT (ml) |
500 |
350 |
350 |
|
V'E (l/min) |
7 |
7 |
9.8 |
|
V'alv (l/min) |
4.7 |
3.4 |
4.7 |
|
V'CO2 (ml/min) |
232 |
232 |
232 |
|
PetCO2 (mmHg) |
39 |
62 |
44 |
|
PaCO2 (mmHg) |
40 |
70 |
46 |

Learn how to interpret a volumetric capnogram and get an overview of the benefits and clinical applications of volumetric capnography. Includes a self-test!