A volumetric capnogram's phases, shape and curve morphology, and calculation derived measurements, can tell you an important story about:
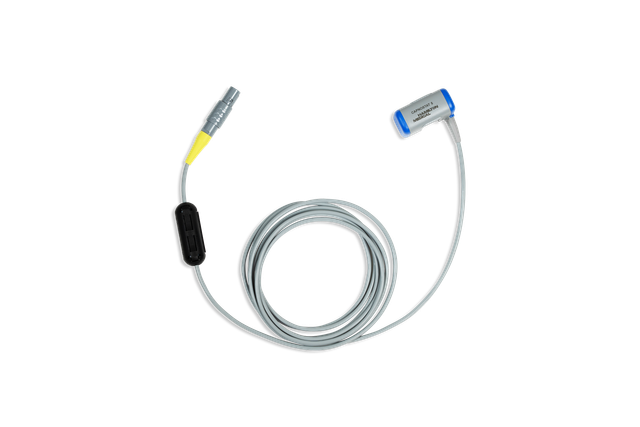
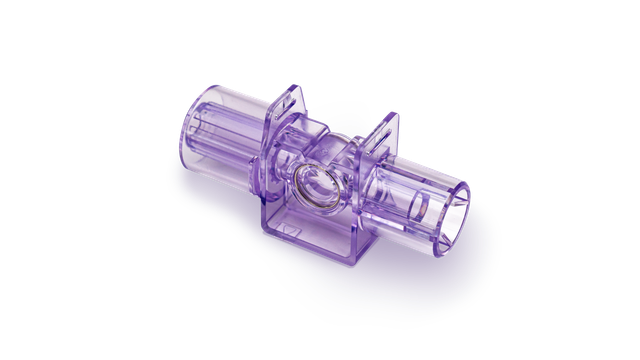
On our ventilators, CO2 is measured with a CAPNOSTAT-5 mainstream CO2 sensor proximal to the patient's airway.
The CAPNOSTAT-5 sensor gives you precise measurements of end-tidal carbon dioxide (PetCO2), and a clear, accurate capnogram at all respiratory rates of up to 150 breaths per minute.
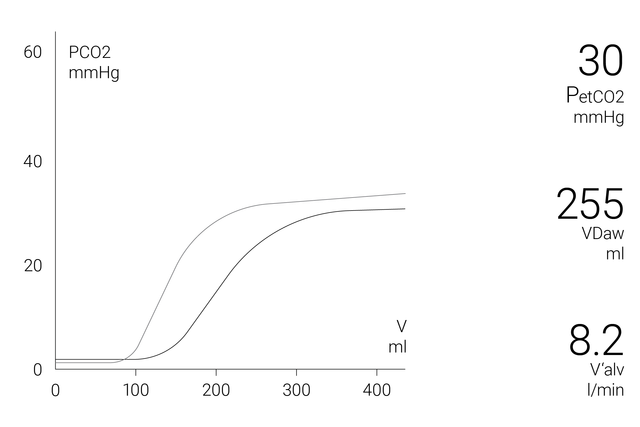
The volumetric capnogram window on the display shows exact quantitative information as a combination of proximal flow and proximal CO2 data such as:
To allow a more comprehensive analysis of the patient condition, a 72-hour trend (or 96-hour with HAMILTON-G5/S1) is available for:
To make your life easier, Hamilton Medical ventilators offer an overview of all relevant CO2-related values in the Monitoring CO2 window.
Learn how to interpret a volumetric capnogram and get an overview of the benefits and clinical applications of volumetric capnography. Includes a self-test!
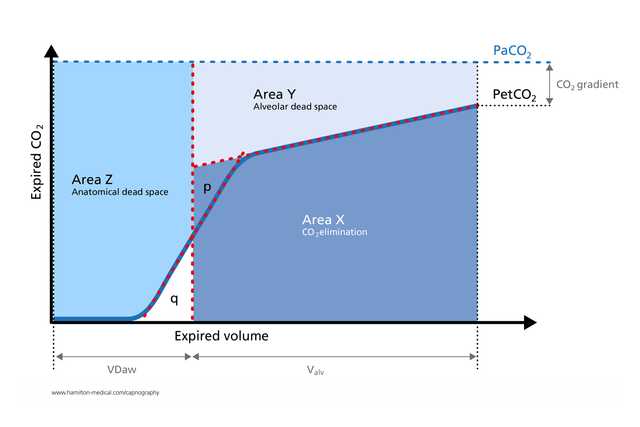
The volumetric capnogram has been used successfully to measure anatomical dead space, pulmonary capillary perfusion, and ventilatory efficiency (
Calculations derived from volumetric capnography are useful for identifying pulmonary embolism at the bedside (
In a study of mechanically ventilated ARDS patients, volumetric capnography measurements of physiologic dead‑space‑to‑tidal‑volume ratio were as accurate as those obtained by metabolic monitor technique (
The expiratory capnogram is an effort‑independent, rapid, and noninvasive measurement that can help detect significant bronchospasms in adult patients with asthma (
By providing valuable real-time insights into the physiology of lung collapse and recruitment in a noninvasive manner, volumetric capnography lends itself to monitoring cyclical recruitment maneuvers at the bedside (

We offer original consumables for adult, pediatric, and neonatal patients. You can choose between reusable and single-use products, according to your institutional policies.
Volumetric capnography is available as an option on the HAMILTON-C6, the HAMILTON-G5, the HAMILTON-C3, and the HAMILTON-C1/T1, and as a standard feature on the HAMILTON-S1.