Estaremos encantados de ayudarle y nos pondremos en contacto con usted lo antes posible.

Nuestro equipo global y nuestros expertos locales están listos para ayudarle.

Acceda a todos los documentos, vídeos, artículos, módulos de formación en línea y recursos adicionales relacionados con todos nuestros productos.

La medición de la presión esofágica (Pes) es un método de monitorización mínimamente invasivo que nos permite determinar la presión transpulmonar.
El método más frecuente de medición de la Pes consiste en utilizar un globo lleno de aire integrado en un catéter esofágico.
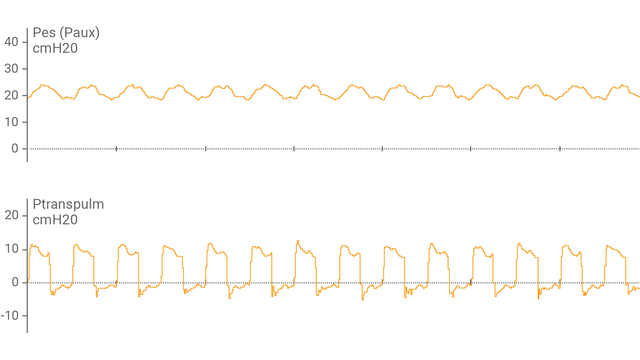
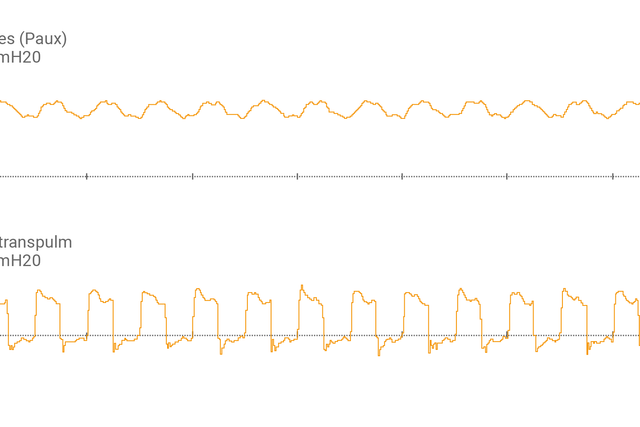
Tras haber conectado el catéter con globo esofágico al puerto auxiliar y haber confirmado su correcta colocación, el respirador muestra la presión esofágica (Pes) y la presión transpulmonar (Ptranspulm) en forma de onda.
Puede medir la Ptranspulm estática utilizando maniobras de pausa inspiratoria y espiratoria.

Para valorar la capacidad de reclutamiento y llevar a cabo maniobras de reclutamiento, la presión transpulmonar también se puede utilizar junto con la herramienta P/V Tool® Pro.

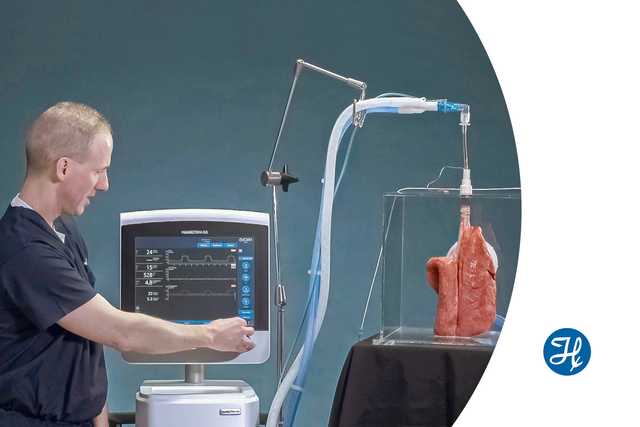
Vea esta pequeña demostración para aprender a utilizar la monitorización de la presión transpulmonar para configurar la PEEP de forma más precisa.


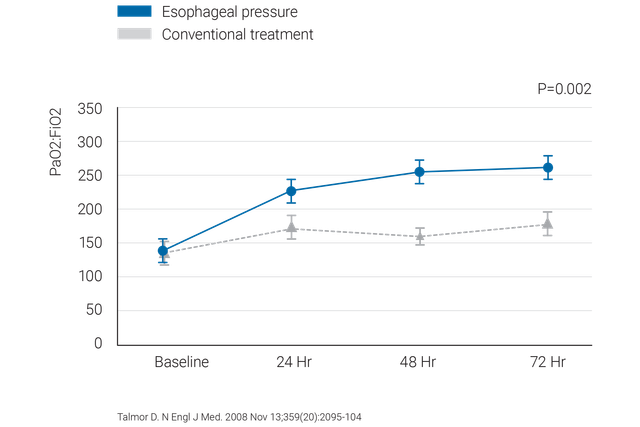
Recomendaciones probadas clínicamente sobre qué hacer y qué evitar a la hora de usar la medición de la presión esofágica en pacientes con SDRA.
Ofrecemos catéteres esofágicos con globo CooperSurgical y catéteres nasogástricos NutriVent.
La monitorización de la presión transpulmonar está disponible como característica estándar en los respiradores HAMILTON-C6 y HAMILTON-G5/S1.