



Autor: Jean-Michel Arnal, Hôpital Sainte Musse, Toulon, Francia
Fecha: 18.09.2025
Last change: 10.06.2026
Typo correctionLa presión de trabajo estática debe monitorizarse sistemáticamente a pie de cama, pero ¿cómo se mide?
En pacientes que reciben ventilación mecánica en los modos de asistencia, la presión de trabajo estática (∆Pstat) se asocia de forma independiente con la supervivencia en la UCI (
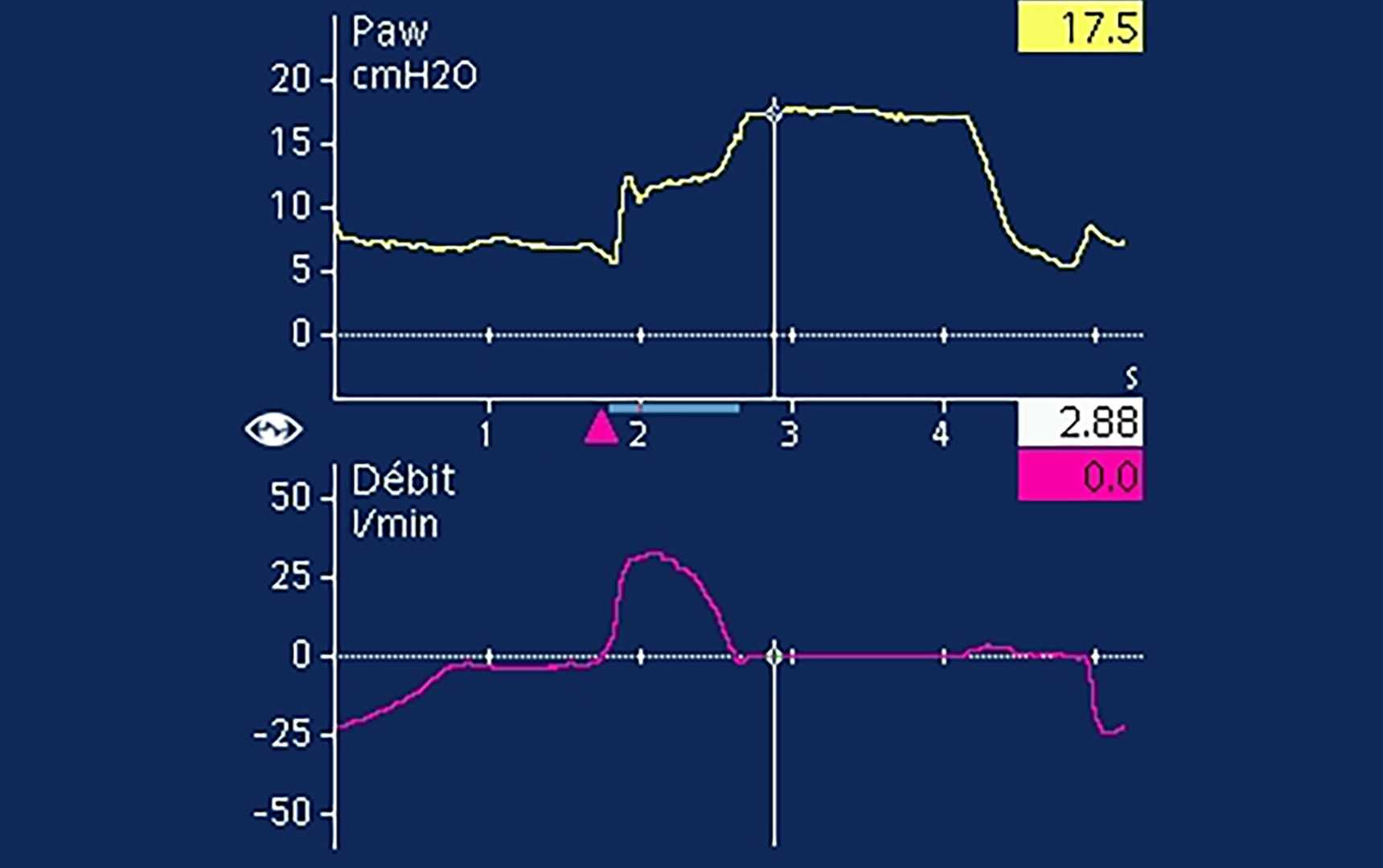
En las respiraciones asistidas, se utiliza una oclusión al final de la inspiración para medir la Pmeseta (

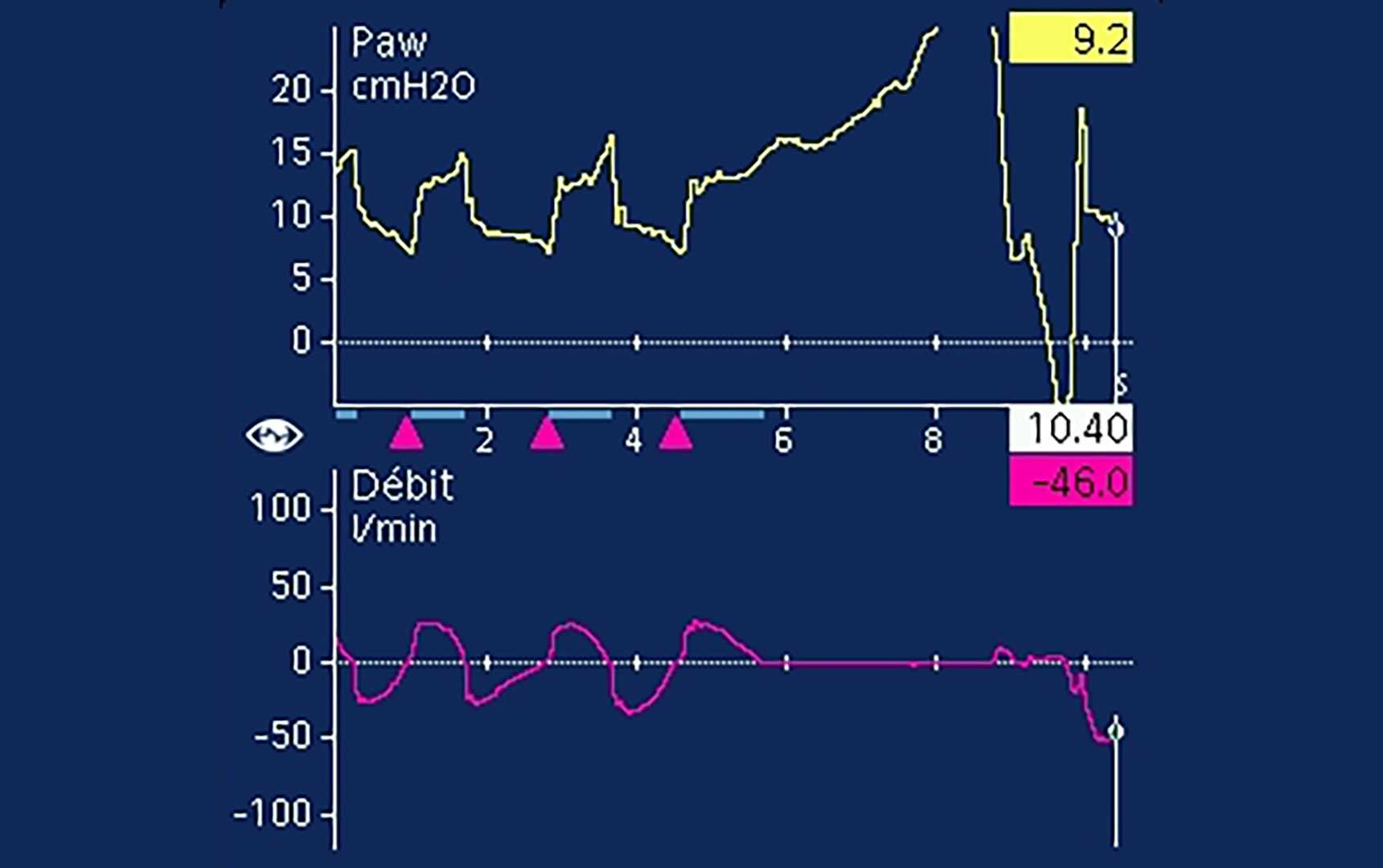

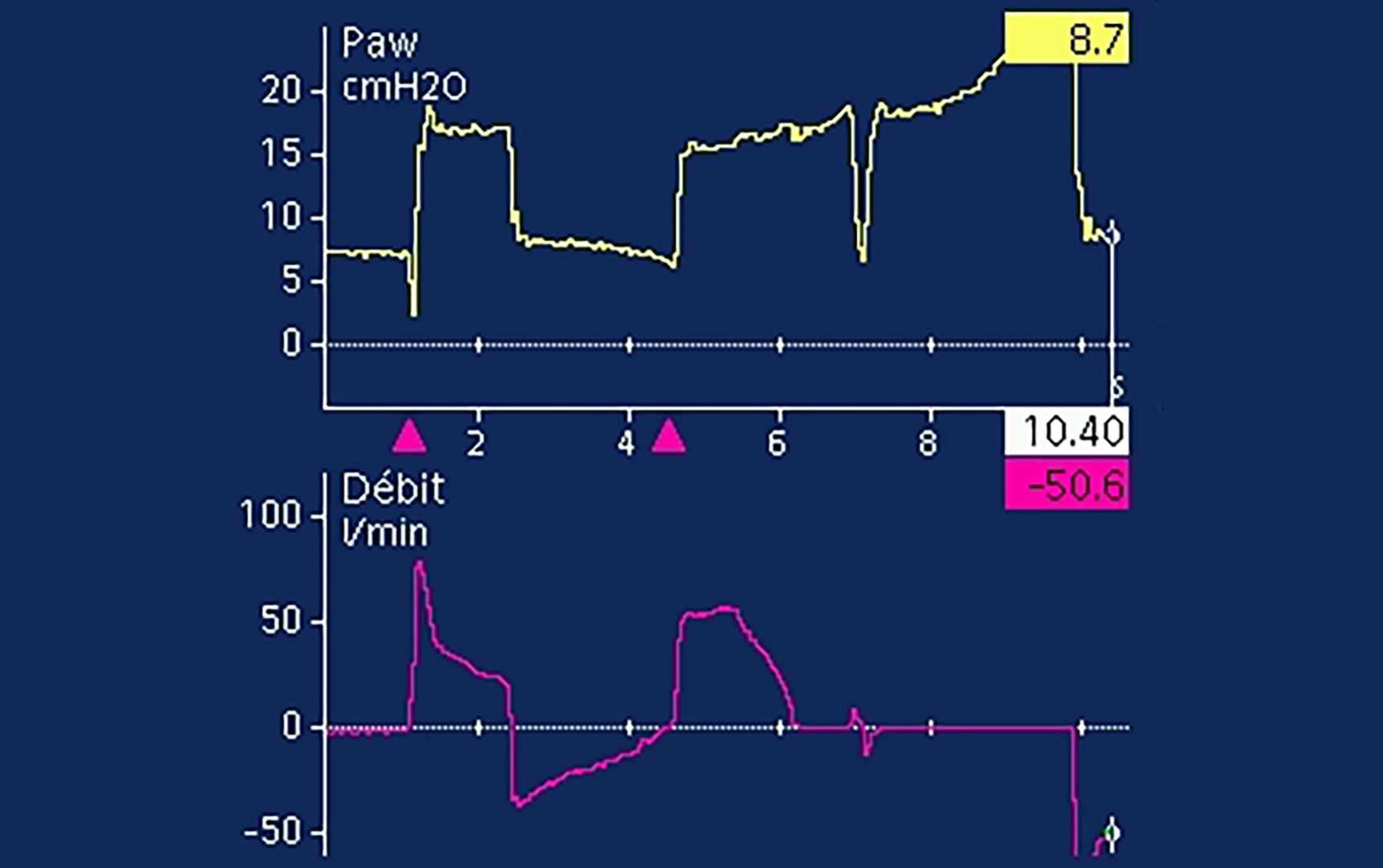
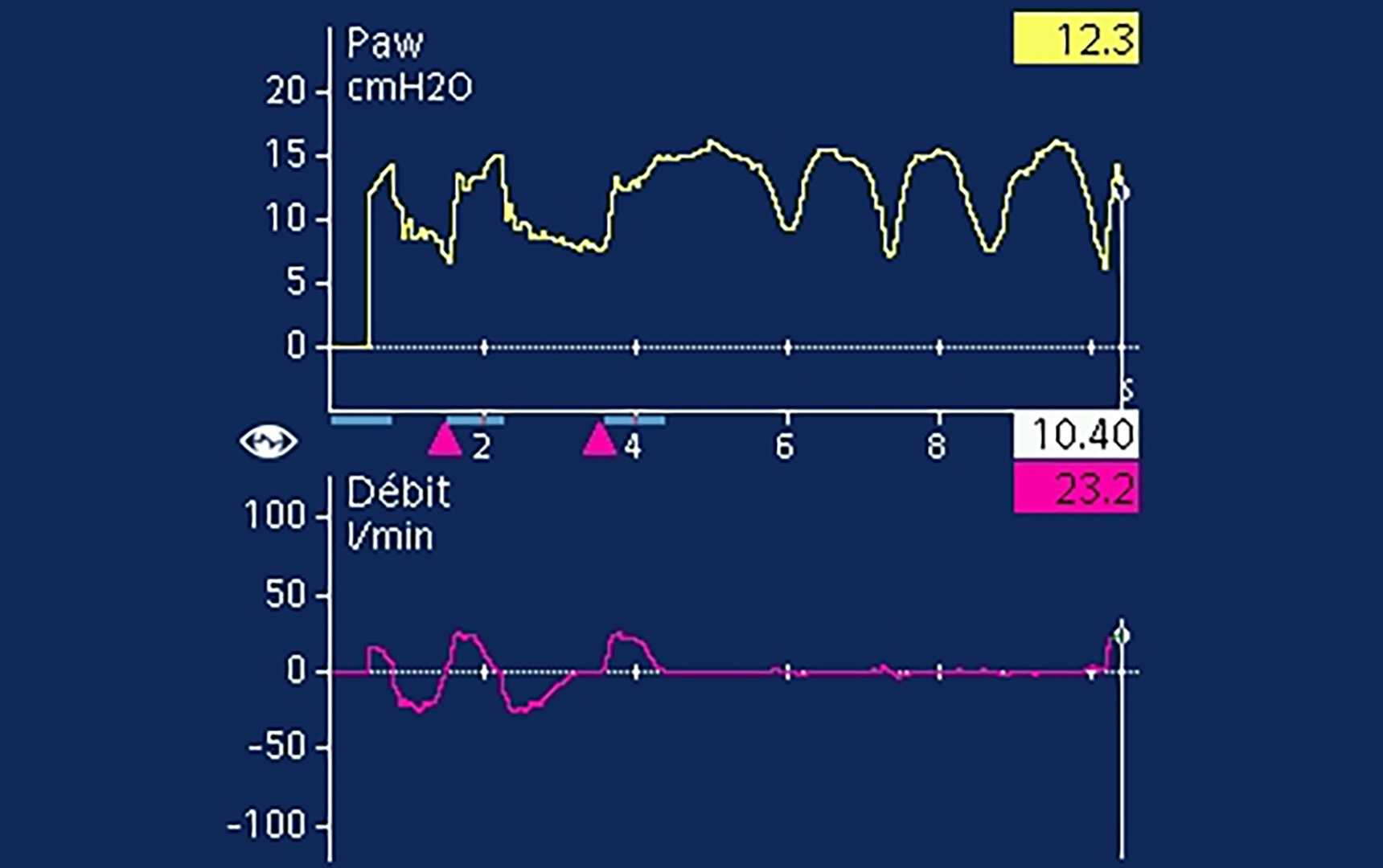
Incluso cuando la meseta es claramente visible, es frecuente que haya actividad de los músculos espiratorios presente (
