


Why is the current volumetric capnogram loop different from the reference loop?
Pulmonary embolism (PE). In the case of PE, there is an increase in alveolar dead space (VDalv) caused by a decrease of blood flow to alveoli that are well ventilated. This gas with low CO2 content is expired in synchrony with gas from normally perfused alveoli. This contrasts with pulmonary diseases affecting the airway, which are characterized by nonsynchronous emptying of compartments with an uneven ventilation/perfusion relationship (

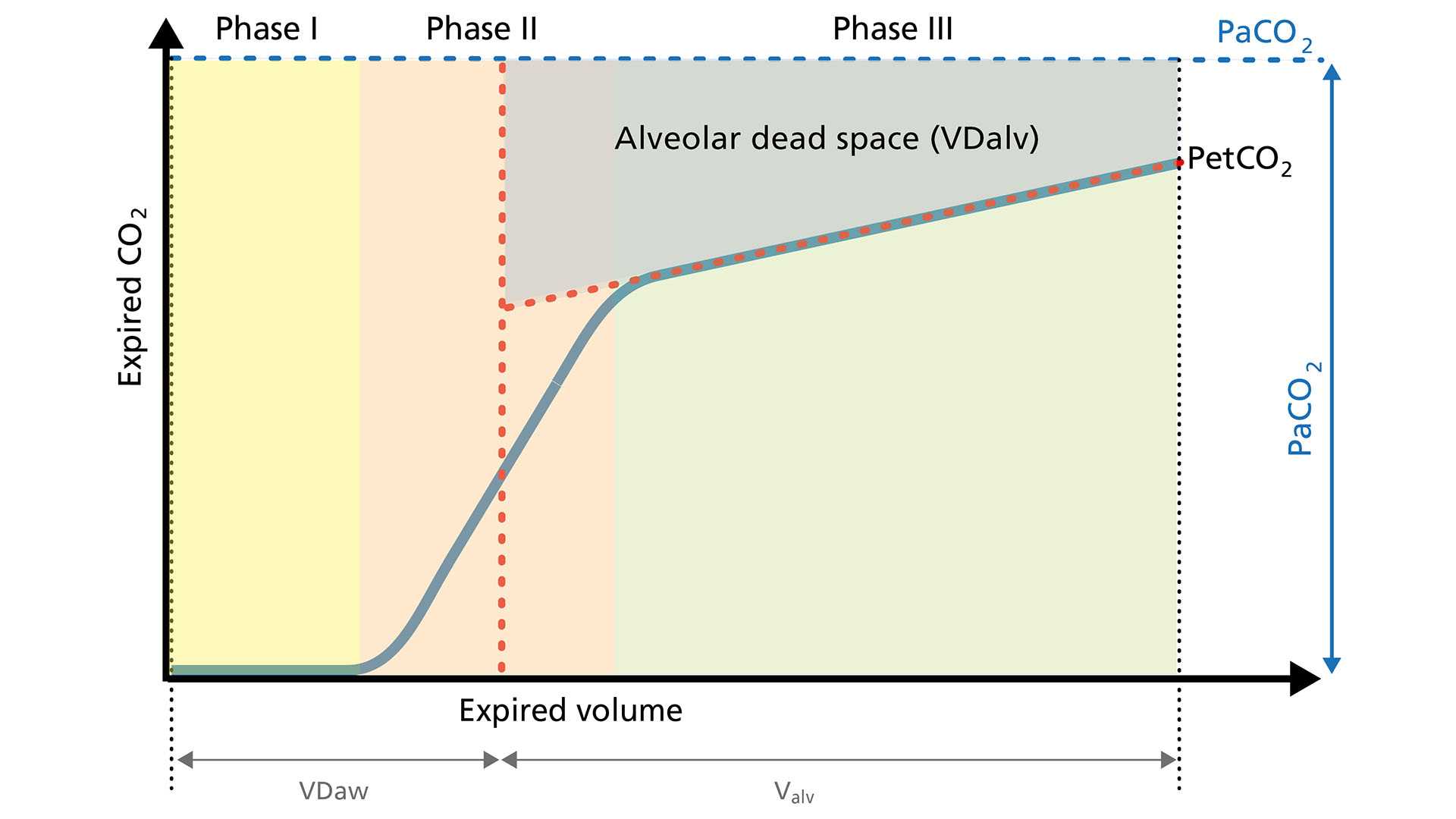
As VDalv increases, the CO2 content of the exhaled gas therefore decreases and causes a consecutive drop in VCO2. The volumetric capnogram loop is characterized by significantly lower PetCO2 and a flatter plateau in Phase III. In addition, the slope in Phase II is less steep.