Auteur: Joe Hylton, MA, BSRT, RRT-ACCS/NPS, NRP, FAARC, FCCM, Clinical Applications Specialist, Hamilton Medical Inc.
Date: 15.07.2021
La capnographie sous formes d'ondes est bien connue des soins intensifs/médecine de soins critiques. Elle est largement utilisée comme outil de validation de gestion des voies aériennes et en sédation consciente, ainsi que pendant le transport intrahospitalier de patients intubés nécessitant une ventilation mécanique. La capnographie sous formes d'ondes peut fournir des informations précieuses en temps utile au personnel soignant bien formé.
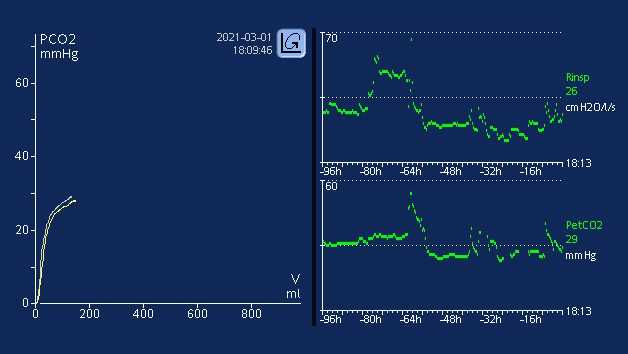
Il existe plusieurs facteurs susceptibles d'affecter la quantité de dioxyde de carbone présente dans le gaz de fin d'expiration (PetCO2). En ce qui concerne l'élimination du CO2, il existe un quasi-équilibre constant entre la production de CO2 dans les tissus, son transport dans le sang, la diffusion dans les alvéoles et l'élimination par la ventilation (
Une augmentation ou une diminution du taux métabolique du patient entraînera une modification de la production de CO2 et, par conséquent, également une élimination du CO2. Si la circulation et la ventilation sont stables (état qui ne peut être obtenu que chez des patients passifs ventilés mécaniquement) le monitorage du CO2 peut servir d'indicateur de la production de CO2. La fièvre, un sepsis, des douleurs et des convulsions constituent tous des conditions susceptibles d'augmenter le métabolisme, provoquant une hausse concomitante de la production de CO2 et, en conséquence, une augmentation de la PetCO2. Une diminution du métabolisme survient chez des patients en hypothermie ou sédatés et paralysés. Cela diminue la production de CO2 et peut entraîner une baisse de la PetCO2 si la ventilation minute n'augmente pas au même moment (
Le transport du CO2 vers les poumons s'appuie sur le bon fonctionnement cardiovasculaire. Par conséquent, tout facteur altérant la fonction cardiovasculaire peut également influer sur le transport du CO2 vers les poumons (
Le rejet du CO2 des poumons dans l'environnement est affecté par des modifications de la fonction respiratoire. Des maladies pulmonaires obstructives, une pneumonie, des troubles neuromusculaires et des troubles du système nerveux central qui entraînent des troubles de la fonction respiratoire impliqueront par conséquent une modification de la valeur de PetCO2 (
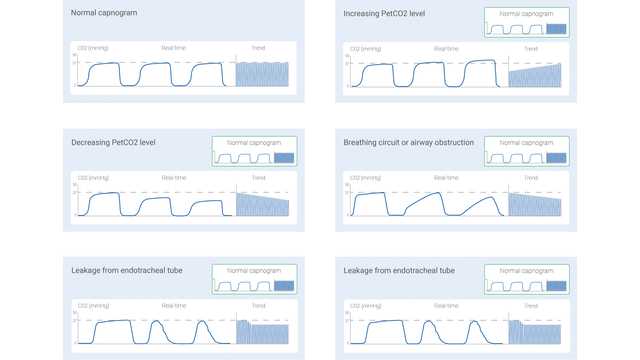
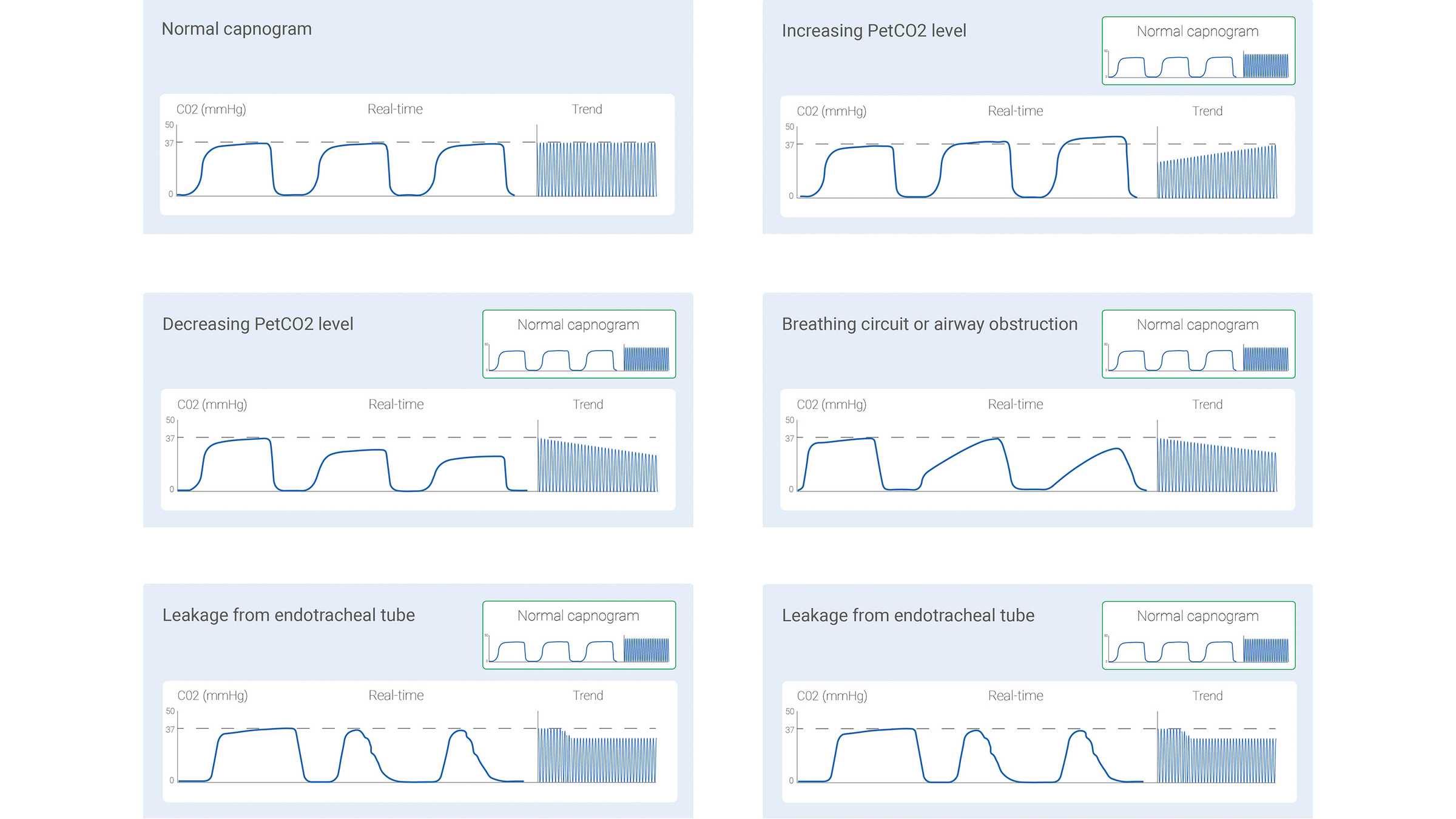
Le signal de CO2 mesuré peut être enregistré soit comme une fonction de temps (capnographie basée sur le temps) soit comme volume expiré (capnographie volumétrique). La quantité d'informations potentiellement fournie par ces deux différents types de capnographie varie considérablement. Certains profils de capnogramme basé sur le temps et considérés comme typiques dans des cas cliniques précis ont été décrits dans la littérature. Certains des cas courants sont représentés ci-dessous à la figure 1.
Cependant, la capnographie basée sur le temps présente également quelques limites : elle ne peut pas fournir d'estimation précise de l'état de ventilation-perfusion des poumons et ne peut pas servir à estimer le composant de l'espace mort physiologique. Même si la capnographie volumétrique n'est pas aussi simple et pratique que la capnographie basée sur le temps, elle présente l'avantage de fournir beaucoup plus d'informations.
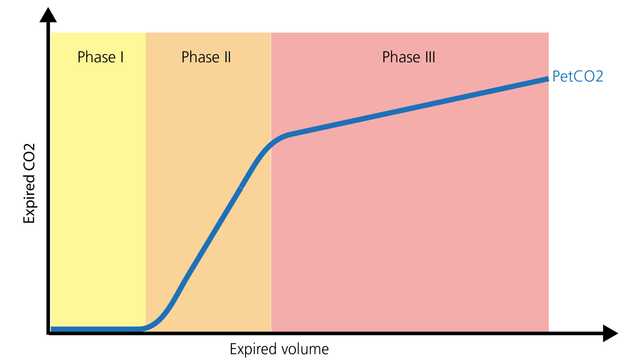
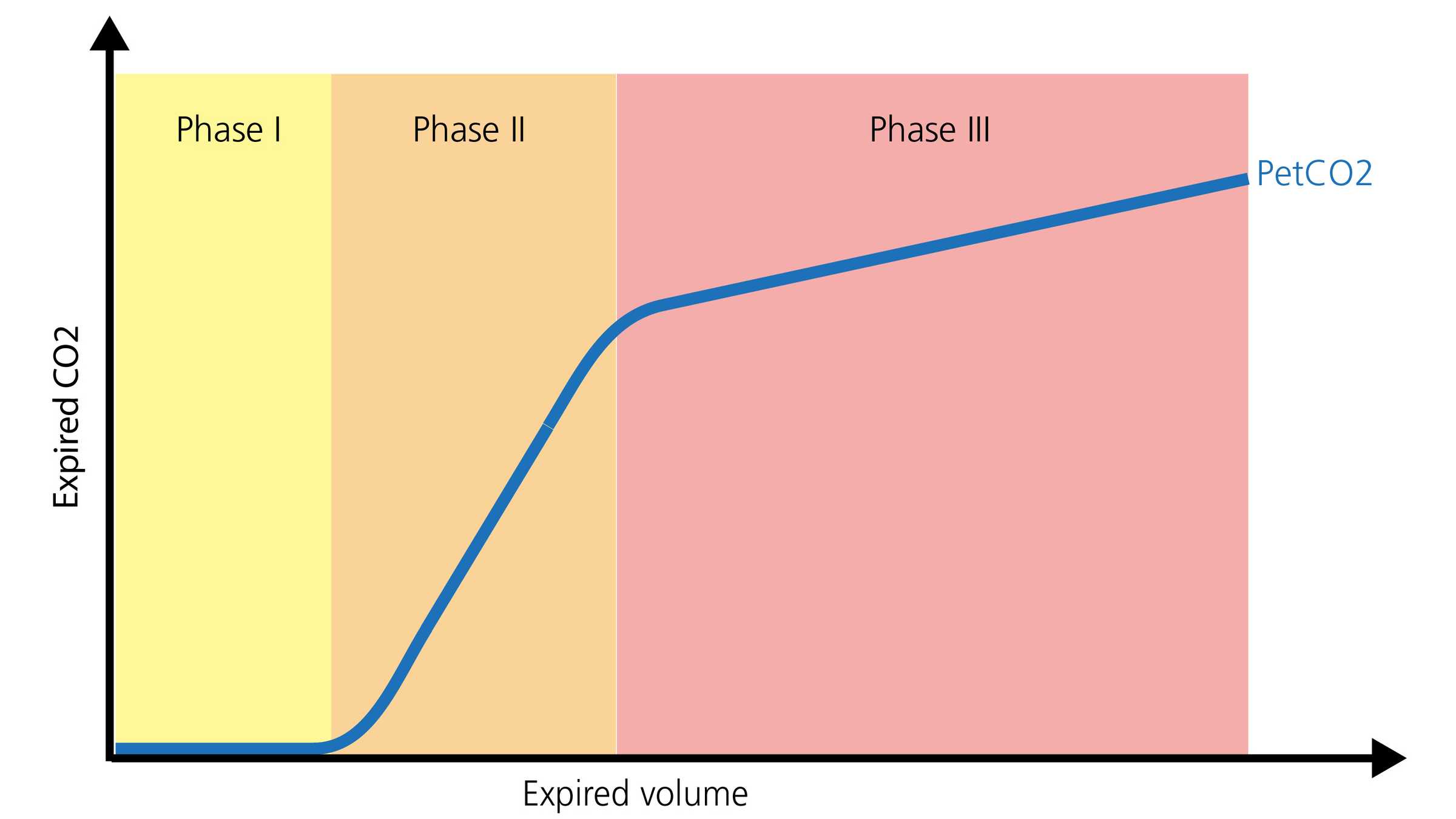
La forme normale d'un capnogramme volumétrique se compose de trois phases. Il est important de se rappeler que le capnogramne est représentatif de l'expiration.
La capnographie, qu'elle soit basée sur le temps ou volumétrique, peut fournir des informations précieuses pour optimiser le monitorage et orienter les soins pour le patient nécessitant un transport intrahospitalier/interhospitalier. Elle peut être utilisée en toute sécurité avec des sondes d'intubation, des canules de trachéotomie et la plupart des voies aériennes supraglottiques, à condition que l'étanchéité soit efficace. La perméabilité et le positionnement des voies aériennes, le monitorage de la ventilation et le statut de la perfusion représentent tous des domaines dans lesquels la PetCO2 fournit des informations importantes. Le volume de dioxyde de carbone éliminé par minute (V'CO2) constitue un autre paramètre précieux ; il permet au personnel soignant d'évaluer l'efficacité de la perfusion et des efforts de réanimation en volume (
En unité de soins intensifs, la capnographie sous formes d'ondes peut continuer le monitorage du positionnement et de la perméabilité des voies aériennes, avec divers dispositifs d'appoint de voies aériennes. Le ratio de l'espace mort par rapport au volume courant (VD/Vt) est une mesure importante de la capnographie. Une augmentation du ratio VD/Vt peut représenter une hausse potentielle de la mortalité, en fonction du degré d'augmentation (
Tous les ventilateurs Hamilton Medical fournissent une capnographie volumétrique (
Apprenez à interpréter un capnogramme volumétrique et découvrez les avantages et les applications cliniques de la capnographie volumétrique. Inclut un auto-test !