



Auteur: Jean-Michel Arnal, Hôpital Sainte Musse, Toulon, France
Date: 18.09.2025
Last change: 10.06.2026
Typo correctionStatic driving pressure should be systematically monitored at the bedside, but how do we measure it?
In mechanically ventilated patients using assisted modes, static driving pressure (∆PSTAT) is independently associated with ICU survival (
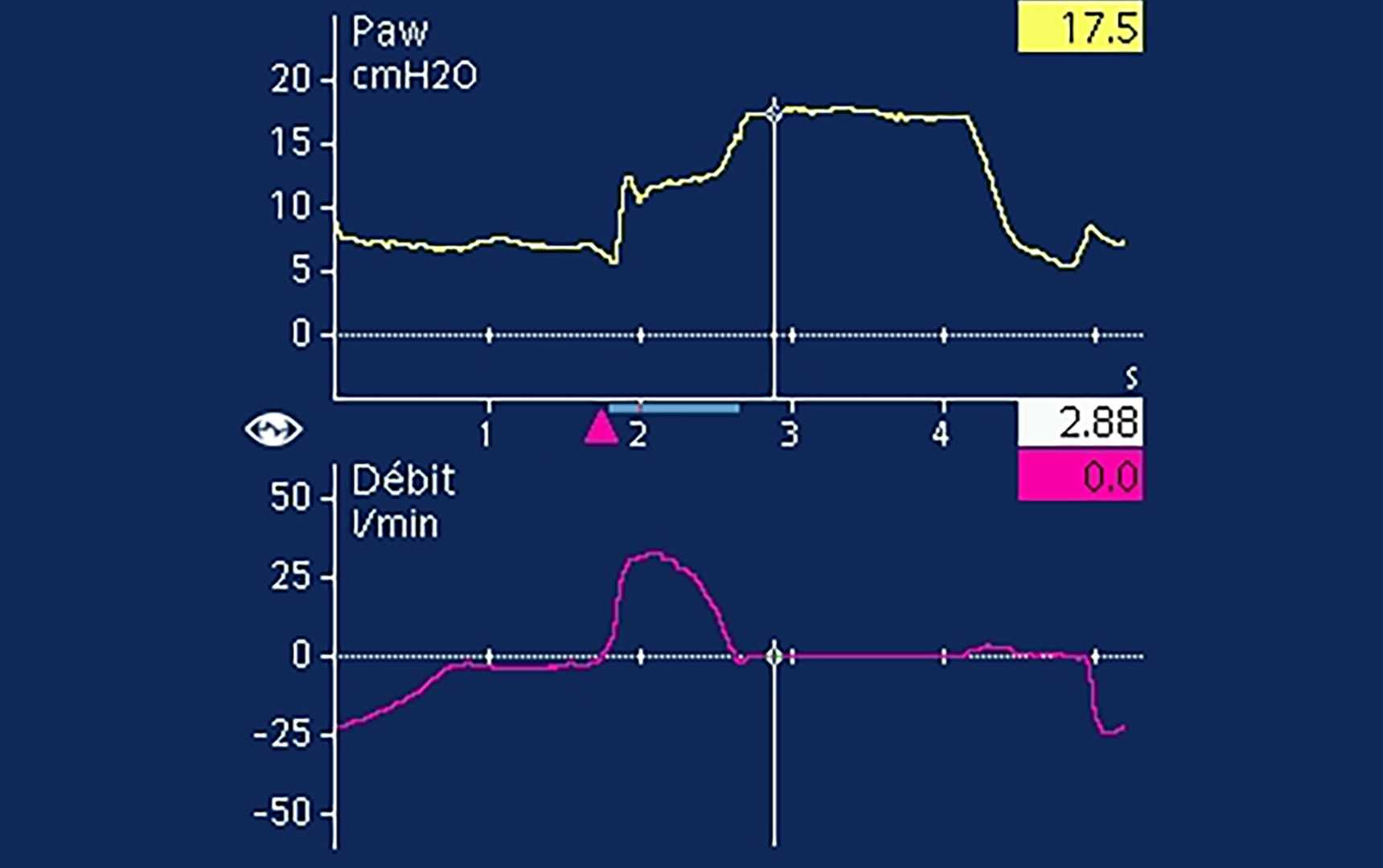
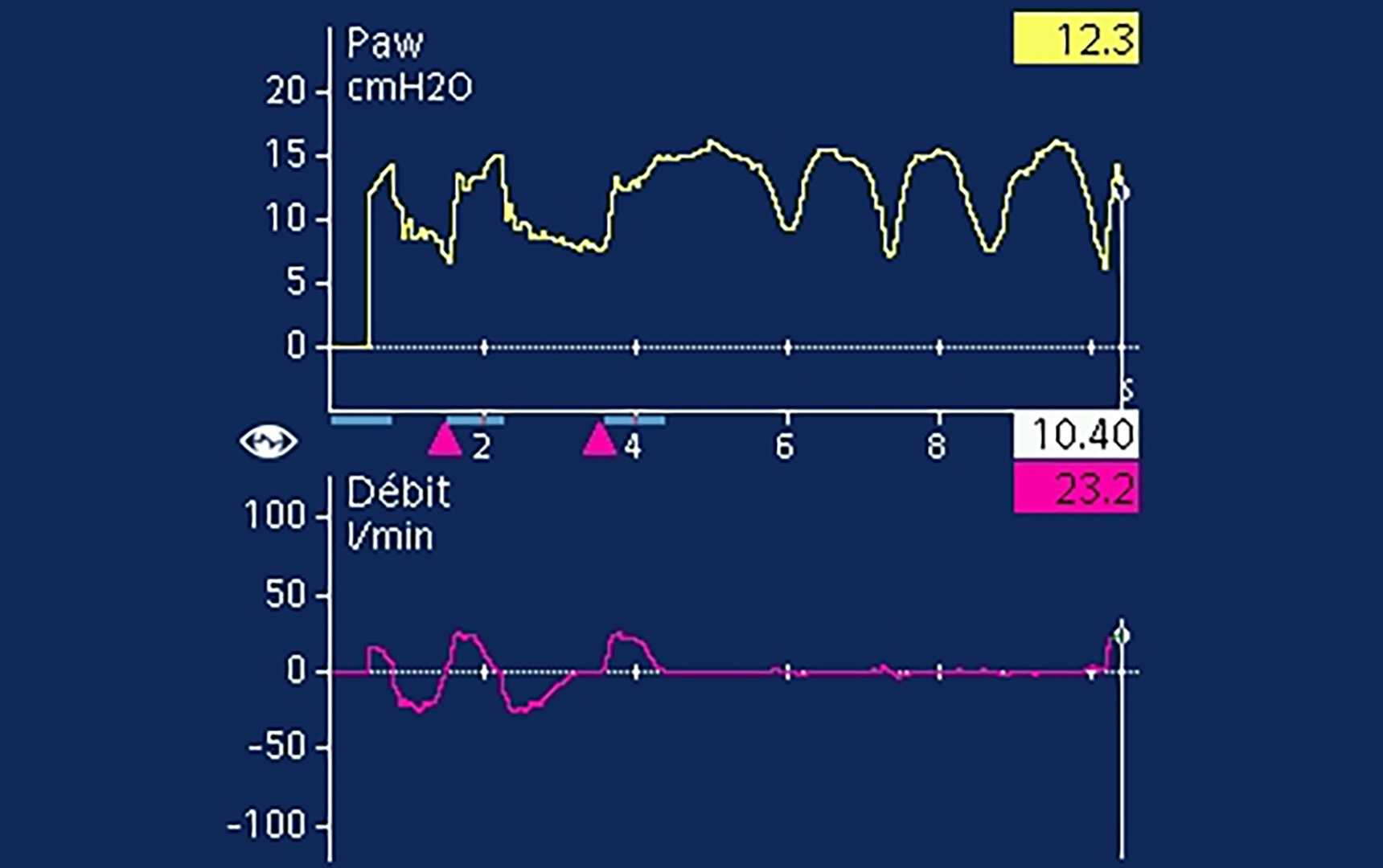
An end-inspiratory occlusion is used to measure PPLAT in assisted breaths (

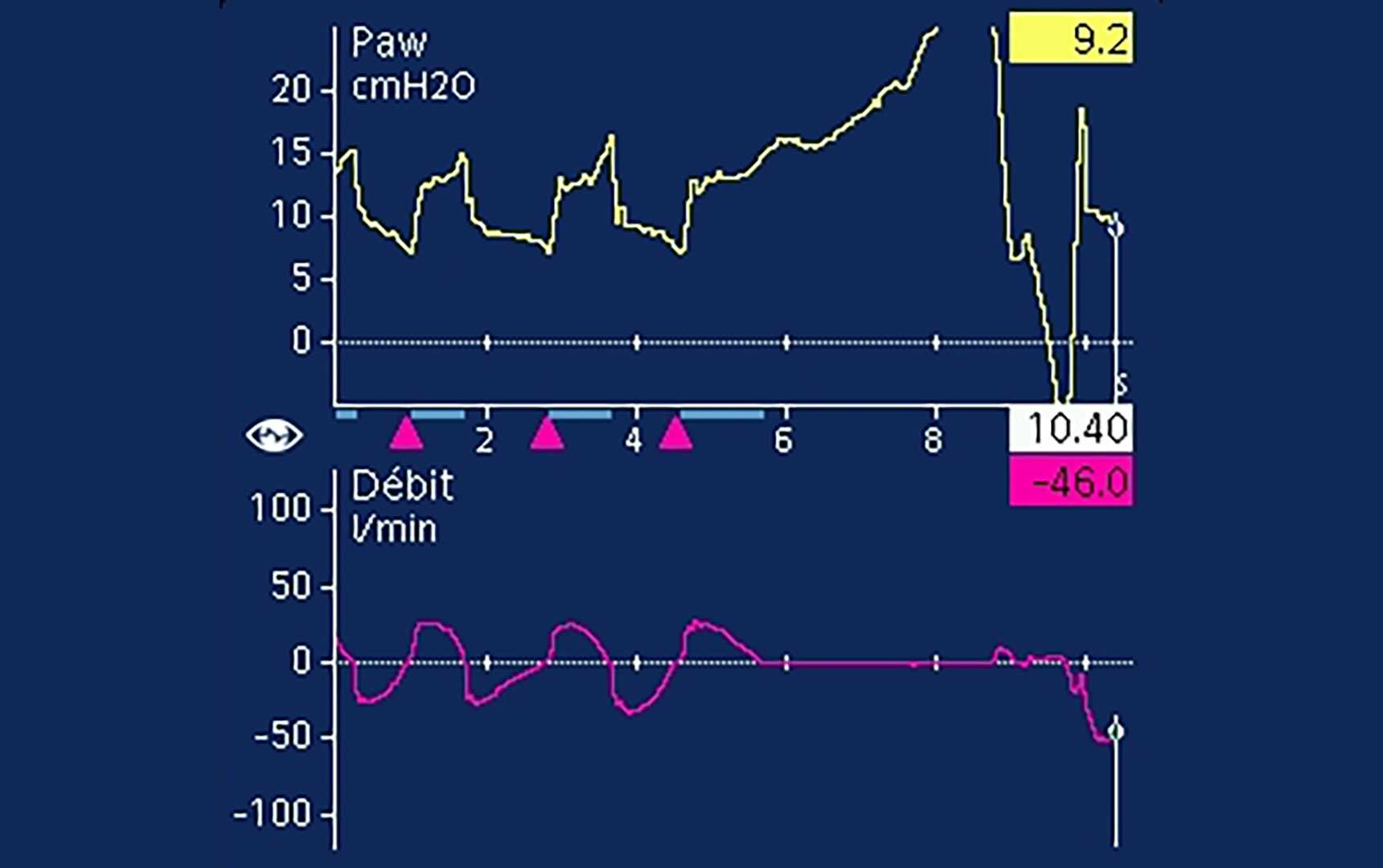

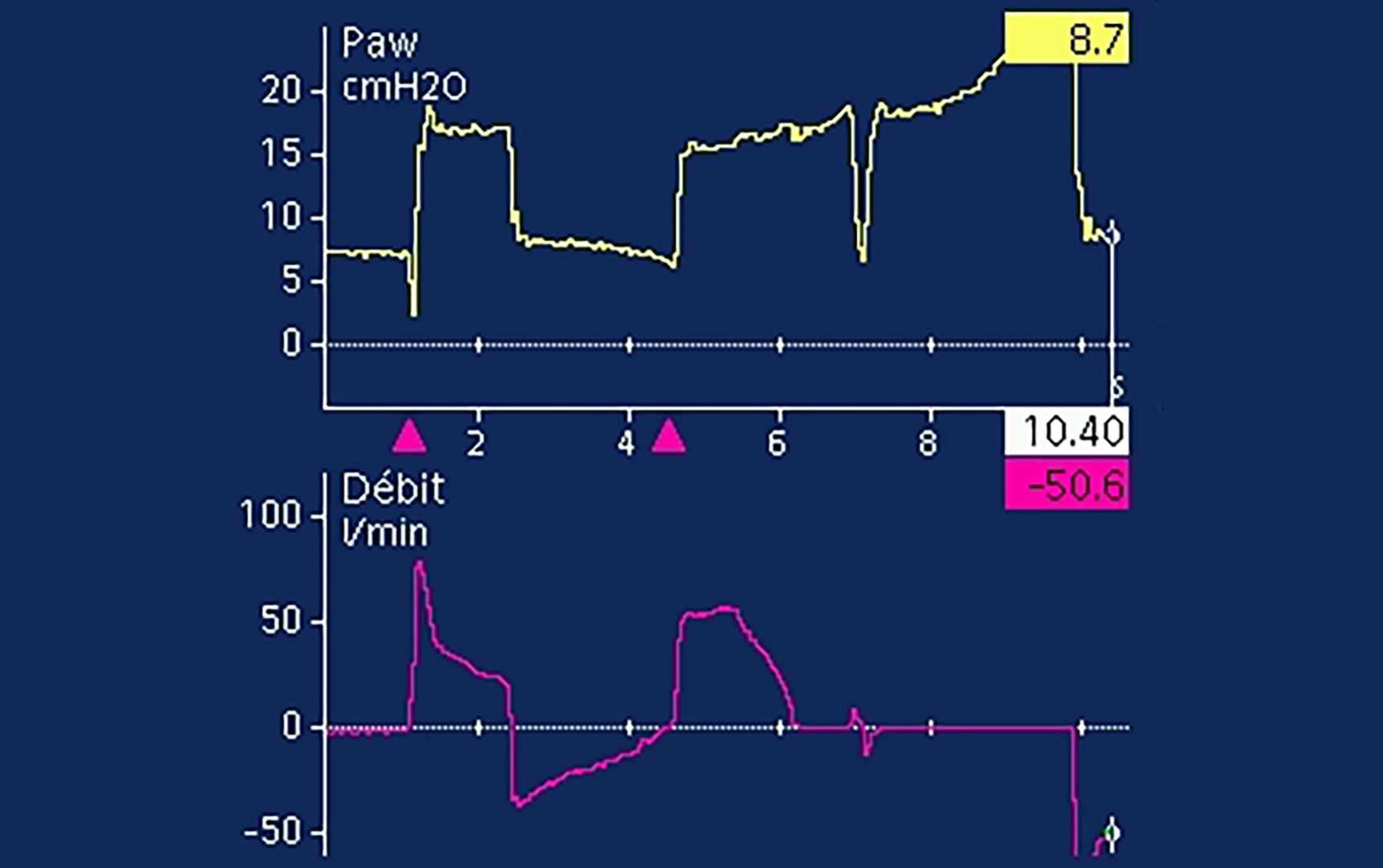
Even when a clear plateau is visible, expiratory muscle activity is frequently present (
