Autore: Joe Hylton, MA, BSRT, RRT-ACCS/NPS, NRP, FAARC, FCCM, Specialista applicazioni cliniche, Hamilton Medical Inc.
Data: 15.07.2021
Le curve capnografiche sono ben note nel campo della medicina intensiva. Sono uno strumento molto utilizzato per confermare la validità dell'approccio alla gestione delle vie aeree e nell'ambito della sedazione cosciente, ma anche durante il trasporto tra una struttura e l'altra dei pazienti intubati e sottoposti a ventilazione meccanica. Le curve capnografiche possono fornire tempestivamente informazioni preziose al personale sanitario correttamente formato.
Sono molti i fattori che possono influenzare la quantità di anidride carbonica presente nel gas espirato nella fase cosiddetta "end-tidal" (PetCO2). Per garantire l'eliminazione della CO2 si ha un equilibrio preciso e continuo tra la produzione di CO2 nei tessuti, il suo trasporto nel sangue, la diffusione negli alveoli e l'eliminazione attraverso la ventilazione (
Un aumento o una riduzione del tasso metabolico del paziente determina una variazione nella produzione della CO2 e, di conseguenza, anche nella sua eliminazione. Se la circolazione e la ventilazione sono entrambe stabili (uno stato che si ottiene solo nei pazienti passivi ventilati meccanicamente) il monitoraggio della CO2 può essere utilizzato come indicatore della produzione della CO2. Febbre, sepsi, dolore e crisi convulsive sono tutte condizioni che aumentano il metabolismo, provocando un corrispondente aumento nella produzione della CO2 e quindi un aumento della PetCO2. Si verifica invece una riduzione del metabolismo nei pazienti ipotermici o sedati e paralizzati. Queste condizioni riducono la produzione di CO2 e possono portare a una diminuzione della PetCO2 se non si ha un contemporaneo aumento della ventilazione minuto (
Il trasporto di CO2 verso i polmoni dipende dal corretto funzionamento del sistema cardiovascolare, quindi qualsiasi fattore che altera la funzionalità cardiovascolare può influenzare anche il trasporto della CO2 verso i polmoni (
La rimozione della CO2 che fuoriesce dai polmoni e viene riversata nell'ambiente è influenzata dalle variazioni della funzionalità respiratoria. Le patologie polmonari ostruttive, la polmonite, i disturbi neuromuscolari e quelli del sistema nervoso centrale che compromettono la funzionalità respiratoria causano quindi una variazione del valore della PetCO2 (
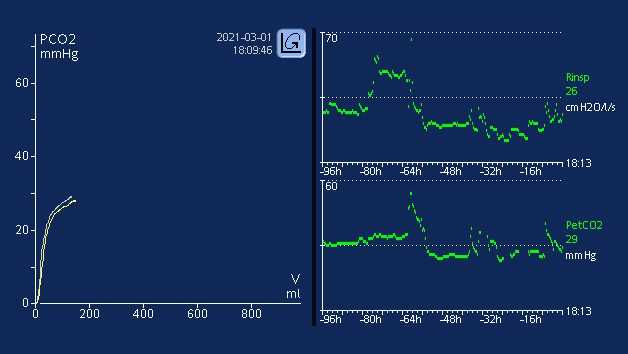
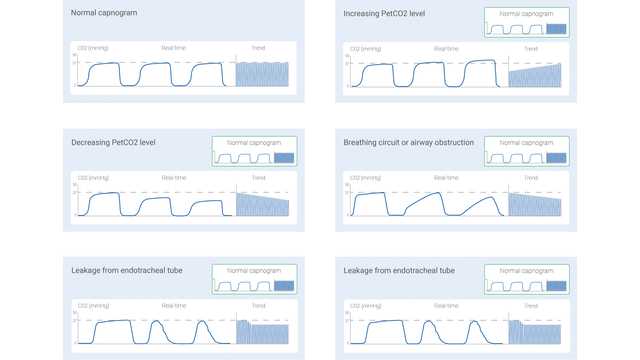
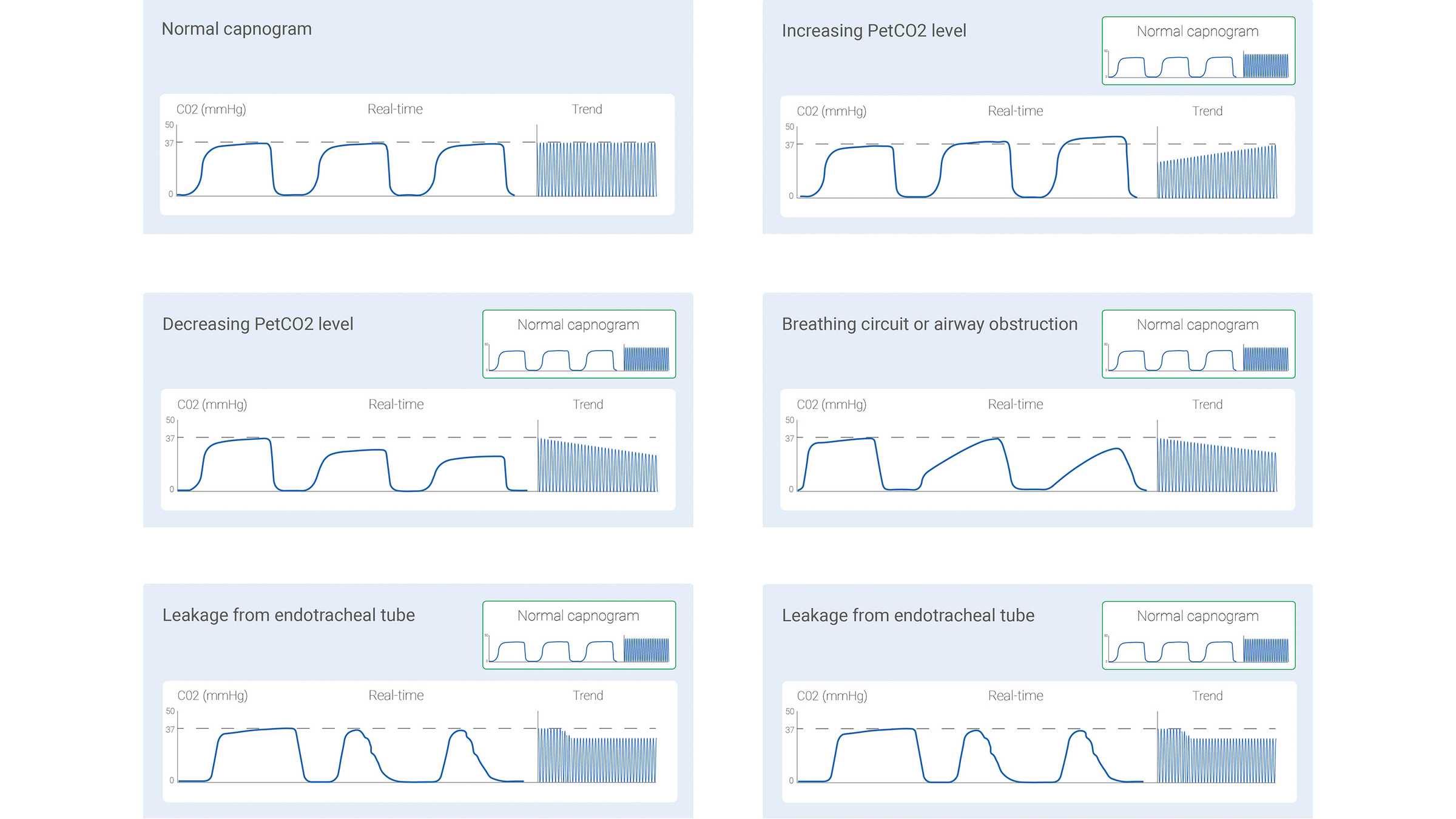
Il segnale di CO2 misurato può essere registrato come funzione del tempo (capnografia basata sul tempo) o del volume espirato (capnografia volumetrica). La quantità di dati potenzialmente forniti da questi due diversi tipi di capnografia varia significativamente. In letteratura sono stati descritti alcuni pattern dei capnogrammi basati sul tempo che vengono ritenuti tipici di determinate situazioni cliniche. Alcuni dei più comuni sono mostrati di seguito, nella Figura 1.
Anche la capnografia basata sul tempo ha però dei limiti: non è in grado di fornire una stima accurata dello stato di ventilazione/perfusione dei polmoni e non può essere utilizzata per fare una stima della componente di spazio morto fisiologico. Nonostante non sia semplice e pratica come la capnografia basata sul tempo, la capnografia volumetrica ha il vantaggio di fornire molte più informazioni.
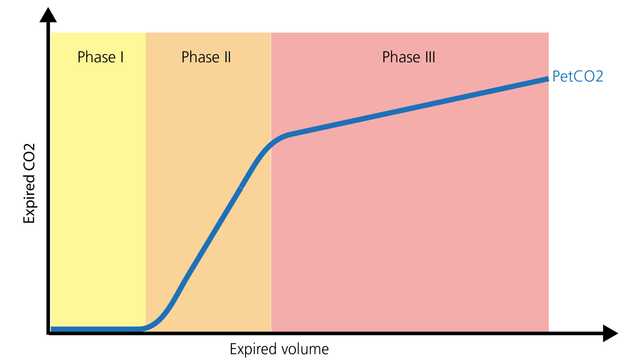
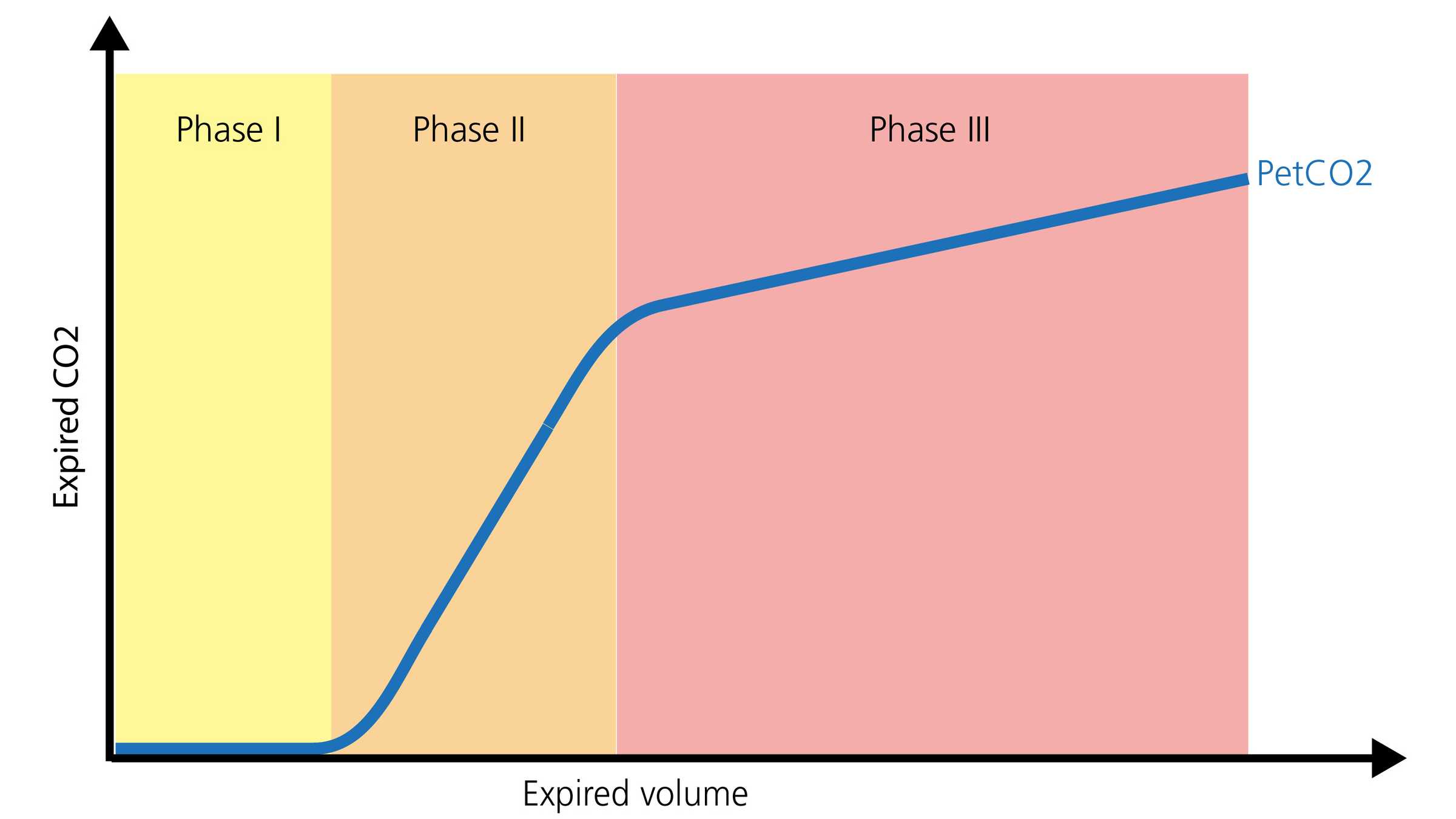
La forma normale di un capnogramma volumetrico è composta da tre fasi. È importante ricordare che il capnogramma rappresenta l'espirazione.
La capnografia, sia essa basata sul tempo o volumetrica, è in grado di fornire informazioni preziose per ottimizzare il monitoraggio e guidare l'assistenza dei pazienti che devono essere trasportati all'interno dell'ospedale o da una struttura a un'altra. Può essere utilizzata in modo sicuro con tubi endotracheali, tubi tracheostomici e molte vie aeree sopraglottiche, purché la tenuta sia efficace. Il posizionamento e la pervietà delle vie aeree, il monitoraggio della ventilazione e lo stato di perfusione sono tutti ambiti in cui la PetCO2 fornisce informazioni significative. Un altro parametro prezioso è il volume dell'anidride carbonica eliminata al minuto (V'CO2), che consente al personale sanitario di valutare l'efficacia della perfusione e gli sforzi di reclutamento del volume (
Nel reparto di terapia intensiva, le curve capnografiche permettono il monitoraggio continuo del posizionamento e della pervietà delle vie aeree, fornendo anche una serie di dati aggiuntivi sulle vie aeree. Il rapporto tra spazio morto e volume corrente (VD/Vt) è un parametro capnografico importante. Un aumento del rapporto VD/Vt può riflettere un potenziale aumento della mortalità, a seconda dell'entità dell'aumento (
Tutti i ventilatori Hamilton Medical eseguono la capnografia volumetrica (
Tutto quel che serve per interpretare un capnogramma volumetrico e avere una panoramica dei vantaggi e delle applicazioni cliniche della capnografia volumetrica. Comprende un test da eseguire in autonomia!