Siamo lieti di aiutarvi e vi ricontatteremo il prima possibile.

Il nostro team globale e gli esperti locali sono pronti a offrire assistenza.

È possibile accedere a tutti i documenti, video, articoli, moduli di e-learning e risorse aggiuntive relative a tutti i nostri prodotti.

La misurazione della pressione esofagea (Pes) è un metodo di monitoraggio mininvasivo che consente di determinare la pressione transpolmonare.
Il modo più comune di misurare la Pes è utilizzare un palloncino pieno d'aria integrato in un catetere esofageo.
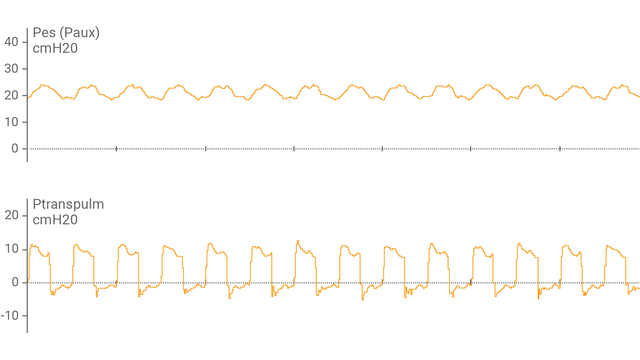
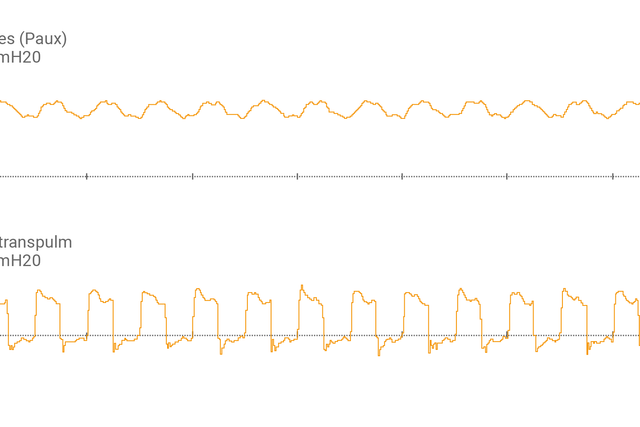
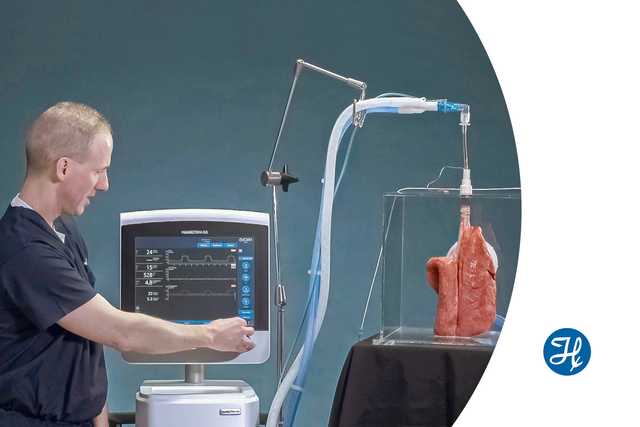
Dopo aver collegato il catetere a palloncino esofageo alla porta ausiliaria e aver verificato che sia posizionato correttamente, è possibile vedere sul display del ventilatore le curve di pressione esofagea (Pes) e pressione transpolmonare (Ptranspulm).
È possibile misurare la Ptranspulm statica utilizzando le manovre di pausa inspiratoria/espiratoria.

Per valutare la possibilità di reclutamento polmonare ed eseguire eventuali manovre di reclutamento, si può anche usare la pressione transpolmonare in combinazione con P/V Tool® Pro.

Questa breve dimostrazione spiega come utilizzare il monitoraggio della pressione transpolmonare per impostare la PEEP in modo più accurato.


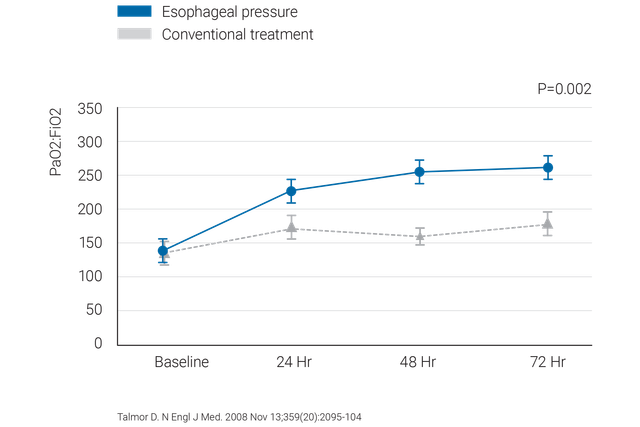
Raccomandazioni comprovate in ambiente clinico su cosa fare e non fare quando si utilizza la pressione esofagea nei pazienti con ARDS.
Mettiamo a disposizione i cateteri a palloncino esofagei CooperSurgical e i cateteri naso-gastrici NutriVent.
Il monitoraggio della pressione transpolmonare è una funzionalità standard sui ventilatori HAMILTON-C6 e HAMILTON-G5/S1.