


Autor: Clinical Experts Group, Hamilton Medical
Data da primeira publicação: 14.07.2017
Última alteração: 30.09.2020
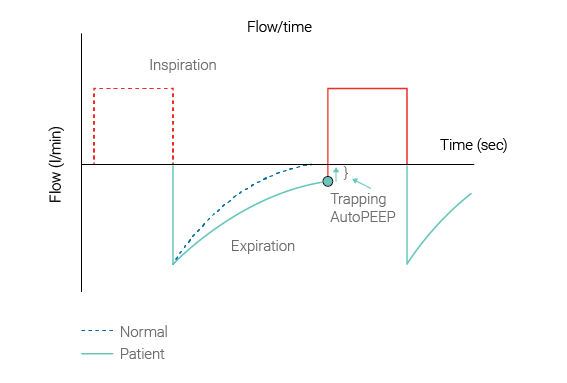
(Originally published 14.07.2017) Previously: select Exp hold, when flow=0 select Exp hold again to deactivate hold maneuver. SW versions updated.Na presença de hiperinsuflação pulmonar dinâmica, a pressão média ao final da expiração dentro dos alvéolos (ou seja, a PEEP real e total (PEEPtot)) é superior à PEEP aplicada pelo respirador (PEEPe). A diferença entre a PEEPtot e a PEEPe corresponde à PEEP intrínseca (PEEPi) também conhecida como AutoPEEP (1).
A autoPEEP também pode ser denominada como retenção de ar, sobreposição de ciclos, hiperinsuflação dinâmica, PEEP indesejada ou PEEP oculta.
A AutoPEEP é um fenômeno comum em pacientes ventilados mecanicamente com constantes de tempo expiratório longas (RCexp), por exemplo, pacientes com doença pulmonar obstrutiva crônica ou asma aguda grave.
IMPORTANTE: A AutoPEEP resultante não pode ser vista na curva de pressão das vias aéreas exibida na tela do respirador durante o fornecimento normal da respiração.
(Figura 1 abaixo: Source Garcia Vicente et al. (

A AutoPEEP predispõe o paciente ao aumento do trabalho respiratório, barotrauma, instabilidade hemodinâmica e dificuldade de acionar o respirador. O não reconhecimento das consequências hemodinâmicas da AutoPEEP pode levar à restrição inadequada de fluidos ou ao tratamento vasopressor desnecessário. A AutoPEEP pode interferir no desmame da ventilação mecânica.
Os prestadores de cuidados devem monitorar se a AutoPEEP ocorre durante a ventilação e definir os parâmetros de controle da ventilação de acordo para evitar as consequências negativas da AutoPEEP.
Todos os respiradores da Hamilton Medical dispõem da capacidade exclusiva de exibir a AutoPEEP como um parâmetro de monitorização com base em cada ciclo respiratório. É calculado aplicando o MMQ a cada ciclo respiratório (
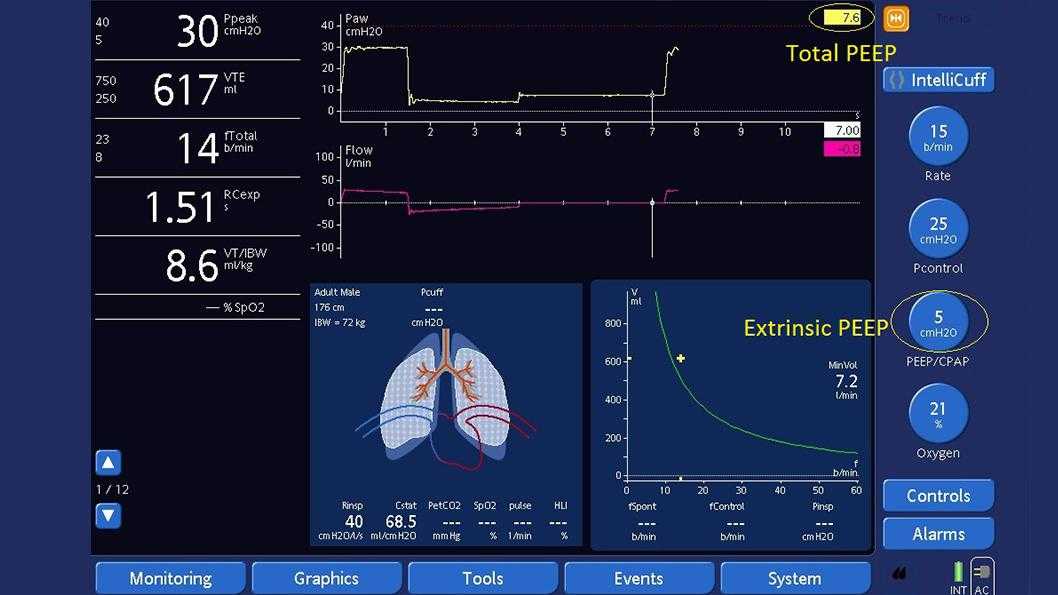
Medindo a PEEP total com uma manobra de pausa expiratória (ver Figura 2 abaixo):
Assegure que a forma de onda Paw é exibida.
| AutoPEEP | '= PEEP total - PEEP extrínseca = PEEP intrínseca |
|---|---|
| PEEP | '= PEEP extrínseca e está pré-selecionada |
| PEEP total | '= PEEP intrínseca + PEEP extrínseca |
Se a AutoPEEP ocorrer acidentalmente, os prestadores de cuidados devem considerar a adaptação dos parâmetros de controle para evitar a retenção de ar, aumentando o tempo de exalação. O uso de tubos endotraqueais de grande diâmetro, broncodilatadores, tempos inspiratórios curtos, tempos expiratórios longos, frequências respiratórias inferiores e o uso de sedativos podem ser necessários para evitar a hiperinsuflação dinâmica causada pela retenção de ar.
Todos os respiradores Hamilton Medical possuem o modo de ventilação inteligente, Ventilação de Suporte Adaptativo (ASV®). O ASV inclui automaticamente estratégias de proteção pulmonar para minimizar complicações da AutoPEEP.
Dispositivos relevantes: HAMILTON-G5/S1 (software v2.8x e posterior); HAMILTON-C3 (software v2.0.x e posterior), HAMILTON-C6 (software v1.1.x e posterior)
Ver a citação completa de (