




Автор: Giorgio Iotti, Caroline Brown
Дата: 29.04.2025
Как рассчитать соотношение R/I на основании данных аппарата ИВЛ?
Соотношение R/I позволяет объективно оценить рекрутируемость легких и подобрать индивидуальный уровень PEEP. Метод одиночного дыхательного маневра, описанный Chen и соавторами (
Ниже мы покажем процесс выполнения этой процедуры на аппарате ИВЛ HAMILTON-C6.
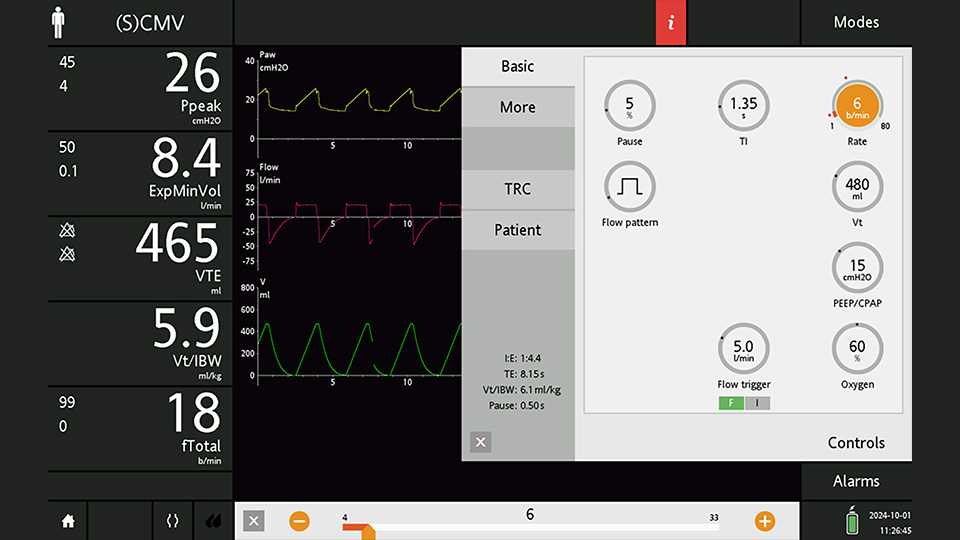
Переведите пациента в режим (S)CMV с PEEP 15 смH2O и поддерживайте его в этом состоянии в течение 30 минут (см. рисунок 1). Установите паузу на вдохе на минимальном уровне в 5 %. Выберите временную шкалу 30 секунд, чтобы к моменту приостановки экрана все важные участки кривых были видимыми.



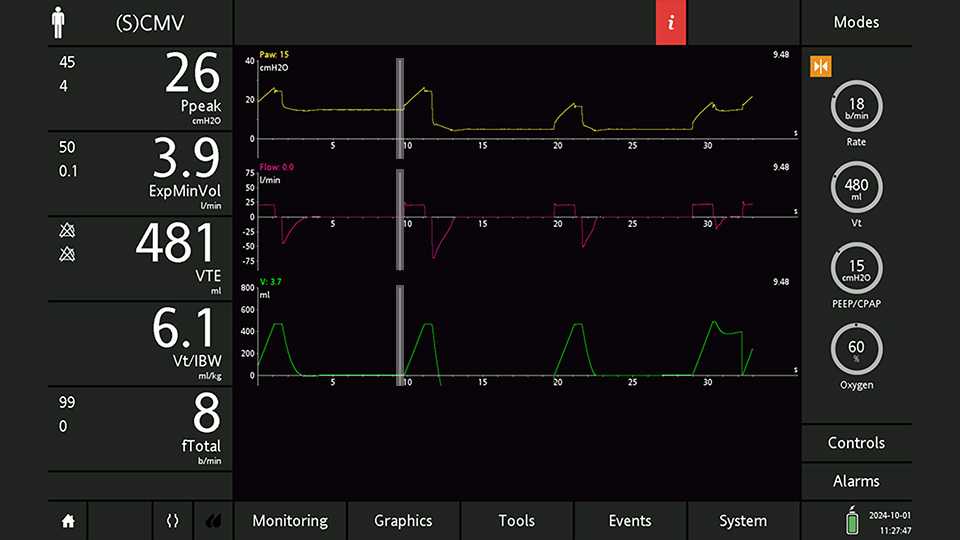
Установите курсор в конец последнего выдоха при высоком уровне PEEP (см. рисунок 5).

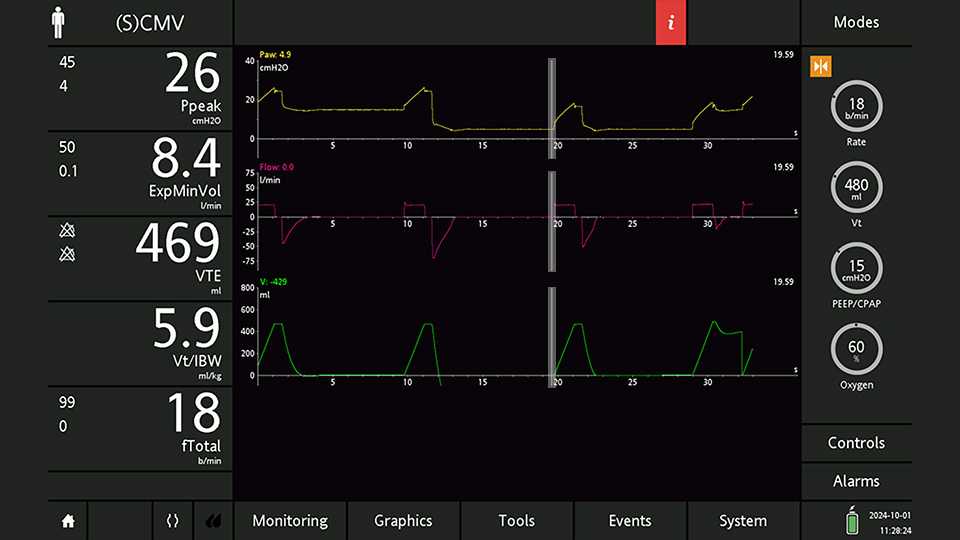
Переместите курсор в конец первого выдоха на более низком уровне PEEP (см. рисунок 6). Здесь измеряется фактическое значение PEEP, низкий и конечно-экспираторный объем относительно исходной линии (значение End-exp Vol, которое не отображается кривой, но считывается курсором). Дополнительный выдыхаемый объем (VTe,plus), вызванный падением альвеол и их дерекрутментом, является противоположным значению End-exp Vol.
Теперь можно рассчитать разницу в PEEP:

Переместите курсор в конец первого инспираторного плато на более низком уровне PEEP (см. рисунок 7). Здесь измеряется давление плато (Pплато,низк.) и инспираторный дыхательный объем (VTi,низк.).
Теперь можно рассчитать минимальное давление вдоха и податливость на более низком уровне PEEP:
После выполнения измерений, описанных в шагах 1, 2 и 3, не забудьте проверить настройку PEEP. Для измерения соотношения R/I необходим всего одно дыхательное движение при более низком уровне PEEP. Продолжение вентиляции при более низком уровне PEEP может вызвать обширный альвеолярный коллапс и, как следствие, серьезное ухудшение обмена газов.


Используя записанные значения, вы можете рассчитать изменения объема, вызванные исключительно инфляцией альвеол (Vinflated), и изменения, связанные с рекрутментом альвеол (Vrecruited).
Эти два значения позволяют вычислить соотношение рекрутмента к инфляции.
Соотношение R/I ниже 0,3 –0,4 свидетельствует о низкой способности к рекрутменту. В этом случае низкий уровень PEEP (от 5 до 8 смH2O) может быть более подходящим выбором. С другой стороны, уровень PEEP не менее 12 смH2O рекомендуется использовать, когда соотношение R/I более 0,6 – 0,7, что указывает на высокую способность к рекрутменту. Промежуточные уровни PEEP рекомендуются, когда соотношение R/I составляет около 0,5 (
