Автор: Дэвид Грумс
Дата: 08.07.2019
В результате изучения частоты асинхронии выяснилось, что они возникают хотя бы один раз не менее чем у 50% пациентов, находящихся на искусственной вентиляции легких (ИВЛ) в течение более 24 часов. Две наиболее распространенные формы асинхронии – это неэффективный (пропущенный) триггер и двойной триггер (ДТ) (
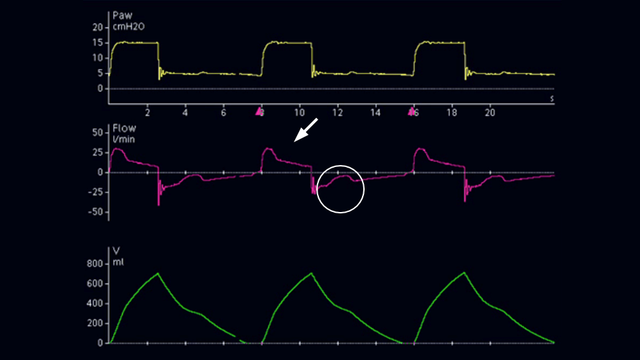
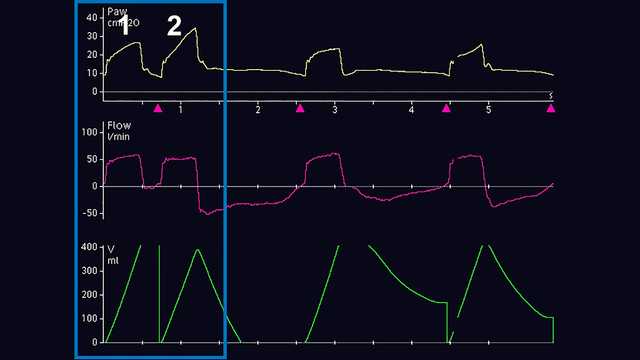
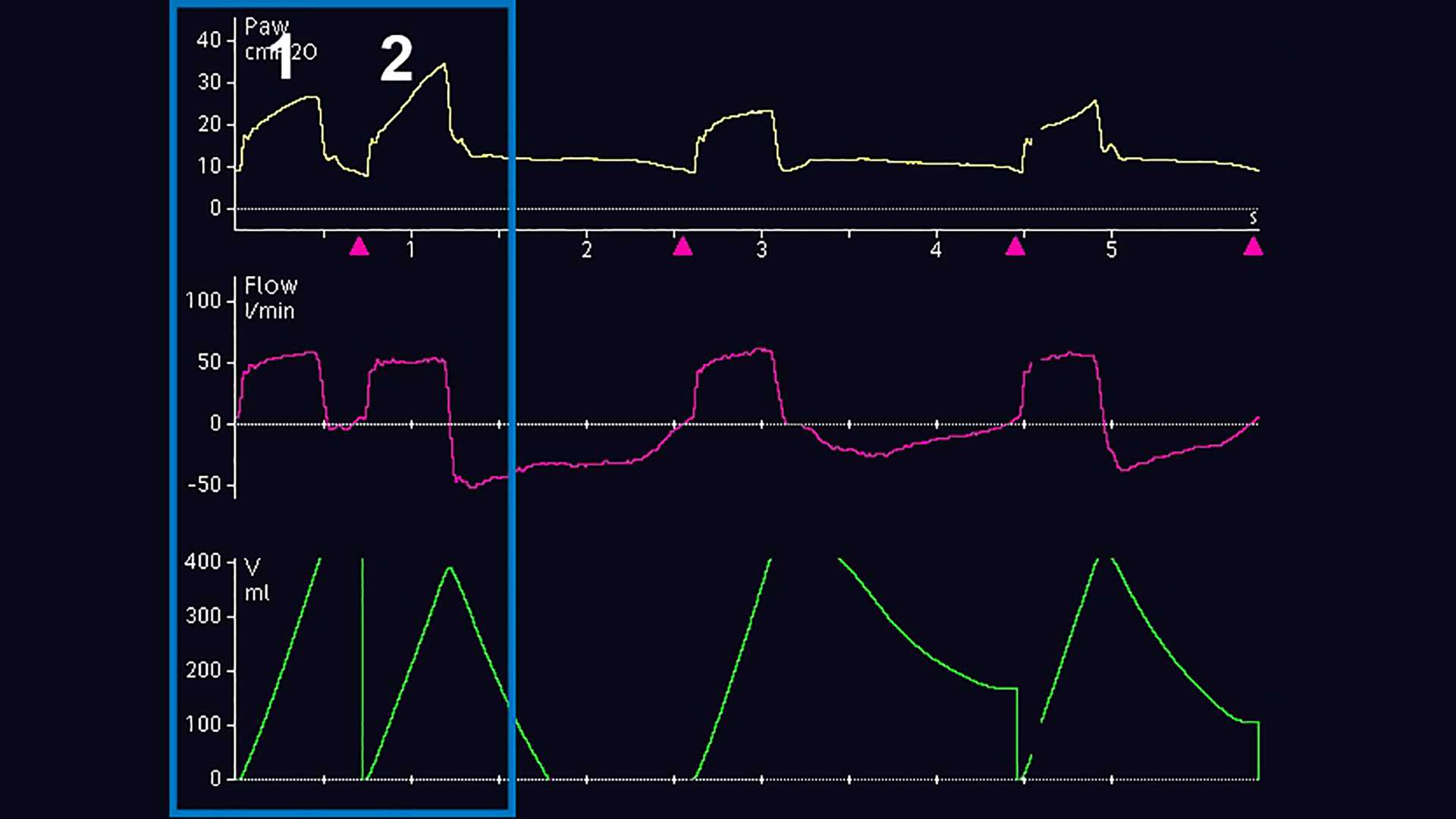
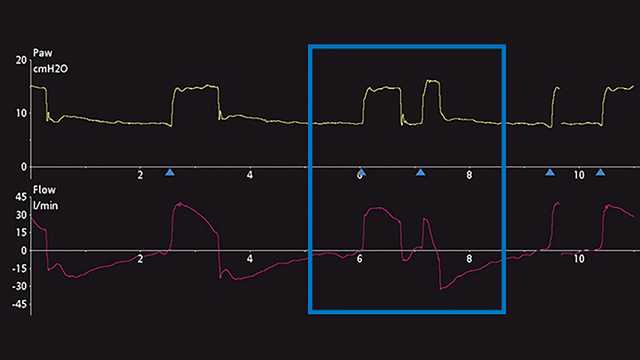
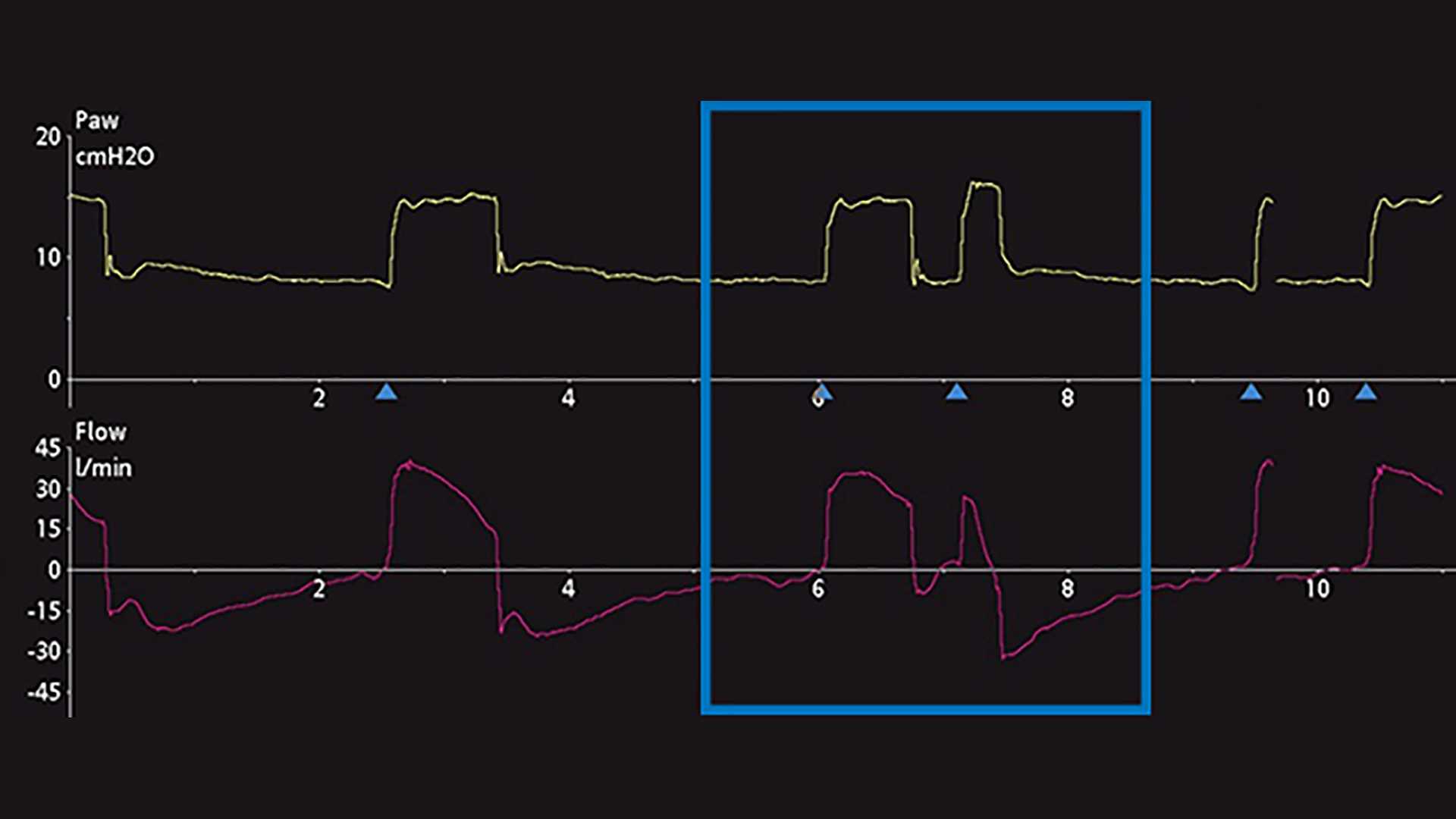
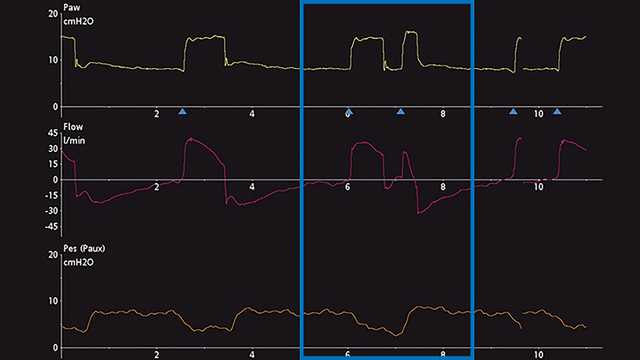
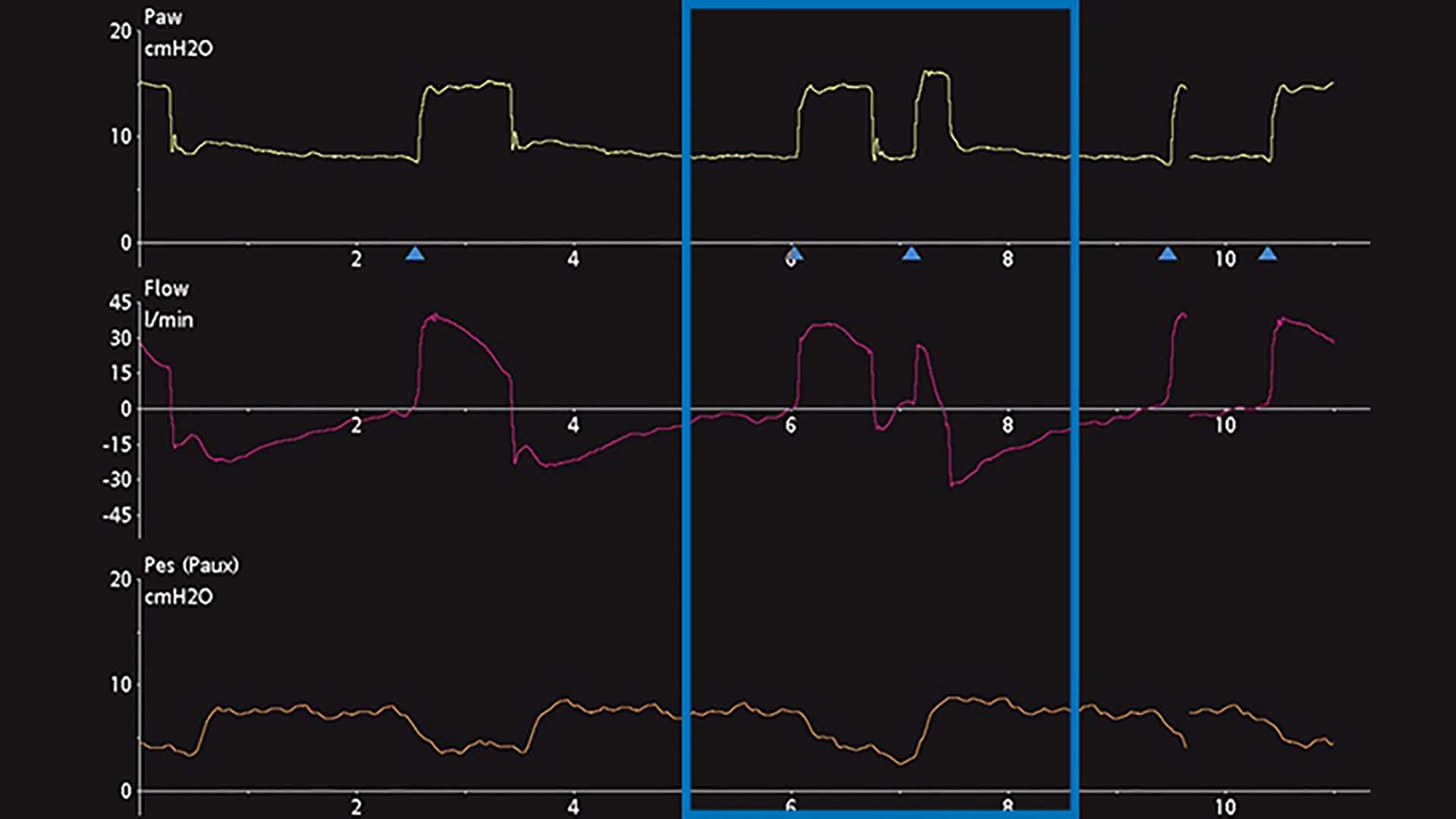
Основным методом обнаружения ДТ является наблюдение и оценка скалярных кривых аппарата ИВЛ. Скалярная кривая – это любая переменная, отображаемая в течение какого-либо времени. На большинстве аппаратов ИВЛ обычно отображаются давление, поток и/или объем в течение какого-либо времени. Чтобы облегчить анализ этих кривых, на некоторых аппаратах ИВЛ отображается пищеводное (приблизительное плевральное) давление в течение какого-либо времени. Этапы правильного распознавания ДТ представлены ниже на снимках экрана аппарата ИВЛ с отображением кривых. На рисунке 1 показаны общие кривые давления, потока и объема, демонстрирующие возникновение ДТ во время инвазивной вентиляции. Сначала неопытному пользователю может быть сложно распознать это явление и правильно определить причину проблемы. Зачастую его ошибочно принимают за второй вдох (вдох 2), самостоятельно сделанный пациентом после подачи аппаратного вдоха (вдох 1) или кислородного голодания. Вследствие этого могут возникнуть серьезные побочные эффекты, если не прекратить искусственную вентиляцию. Поэтому рекомендуется более тщательный анализ с помощью эзофагоманометрии для сравнения и сопоставления плеврального давления и изменений давления и потока в дыхательном контуре аппарата ИВЛ. На следующем снимке ниже показано отображение скалярного времени давления и потока на экране аппарата ИВЛ. Здесь есть тонкий намек на возможный ДТ, но его также можно ошибочно принять за дополнительное дыхательное усилие пациента (рисунок 2). При отображении скалярной кривой пищеводного давления (кривая Pes-Paux) оказывается, что двойной триггер действительно имеется. Он возник из-за последовательной подачи вдохов во время одного дыхательного усилия пациента (см. снижение плеврального давления на рисунке 3).
Дифференциация и классификация типа ДТ также является сложной задачей при лечении пациентов. Текущие исследования показывают, что ДТ можно разделить на три разных типа (
Данные показали, что в фазе, предшествующей вдоху, часто происходит задержка триггрования, составляющая 0,07–0,13 секунды (
Наиболее распространенными причинами ДТ являются неправильное согласование времени аппаратного вдоха и времени нейронального вдоха, а также недостаточный уровень поддержки давлением при высокой активности дыхательного центра (