Автор: Джо Хилтон, врач-консультант, бакалавр наук в области радиологических технологий, аккредитованный специалист по дыхательной терапии у взрослых/педиатрических/неонатальных пациентов, участник программы неонатальной реанимации, член Американской ассоциации искусственной вентиляции легких, член Американской коллегии интенсивной терапии, специалист по клиническим процедурам, компания Hamilton Medical Inc.
Дата: 15.07.2021
Капнография давно известна в области интенсивной терапии и неотложной медицинской помощи. Она широко используется как инструмент контроля уровня кислорода в дыхательных путях и применяется в условиях обезболивания при сохранении сознания, а также во время транспортировки интубированных пациентов, нуждающихся в искусственной вентиляции легких, между больницами. С помощью капнографии хорошо обученный медицинский персонал может получать своевременную и ценную информацию.
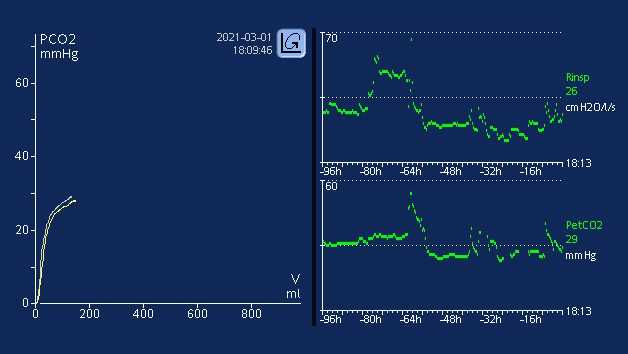
Существует множество факторов, которые могут повлиять на количество углекислого газа в выдыхаемой газовой смеси (PetCO2). Для выведения СО2 существует тесный, непрерывный баланс между выработкой СО2 в тканях, его транспортировкой в крови, диффузией в альвеолы и выведением путем вентиляции (
Повышение или снижение скорости метаболизма пациента приводит к изменениям в выработке CO2, а следовательно, и в выведении CO2. Если и кровообращение, и вентиляция стабильны – состояние, которого можно достичь только у пациентов, находящихся на пассивной искусственной вентиляции легких, – мониторинг CO2 можно использовать в качестве индикатора выработки CO2. Лихорадка, сепсис, боль и судороги – все это состояния, которые ускоряют метаболизм и вызывают соответствующее увеличение выработки CO2 и, в свою очередь, увеличение PetCO2. Снижение скорости метаболизма наблюдается у пациентов, находящихся в состоянии гипотермии, под наркозом или пораженных параличом. В таких состояниях выработка CO2 снижается, что может привести к снижению PetCO2, если одновременно не увеличить минутную вентиляцию (
Поступление CO2 в легкие зависит от правильности функционирования сердечно-сосудистой системы; следовательно, любой фактор, который влияет на функции сердечно-сосудистой системы, также может влиять на поступление CO2 в легкие.(
На выведение CO2 из легких в окружающую среду влияют изменения в дыхательной функции. Таким образом, обструктивные заболевания легких, пневмония, нервно-мышечные нарушения и заболевания центральной нервной системы, приводящие к нарушению дыхательной функции, влияют на изменение значения PetCO2 (
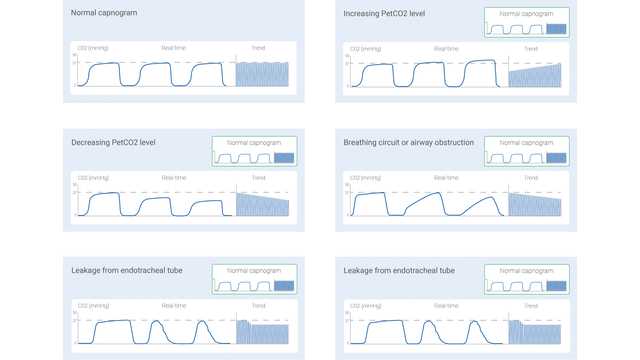
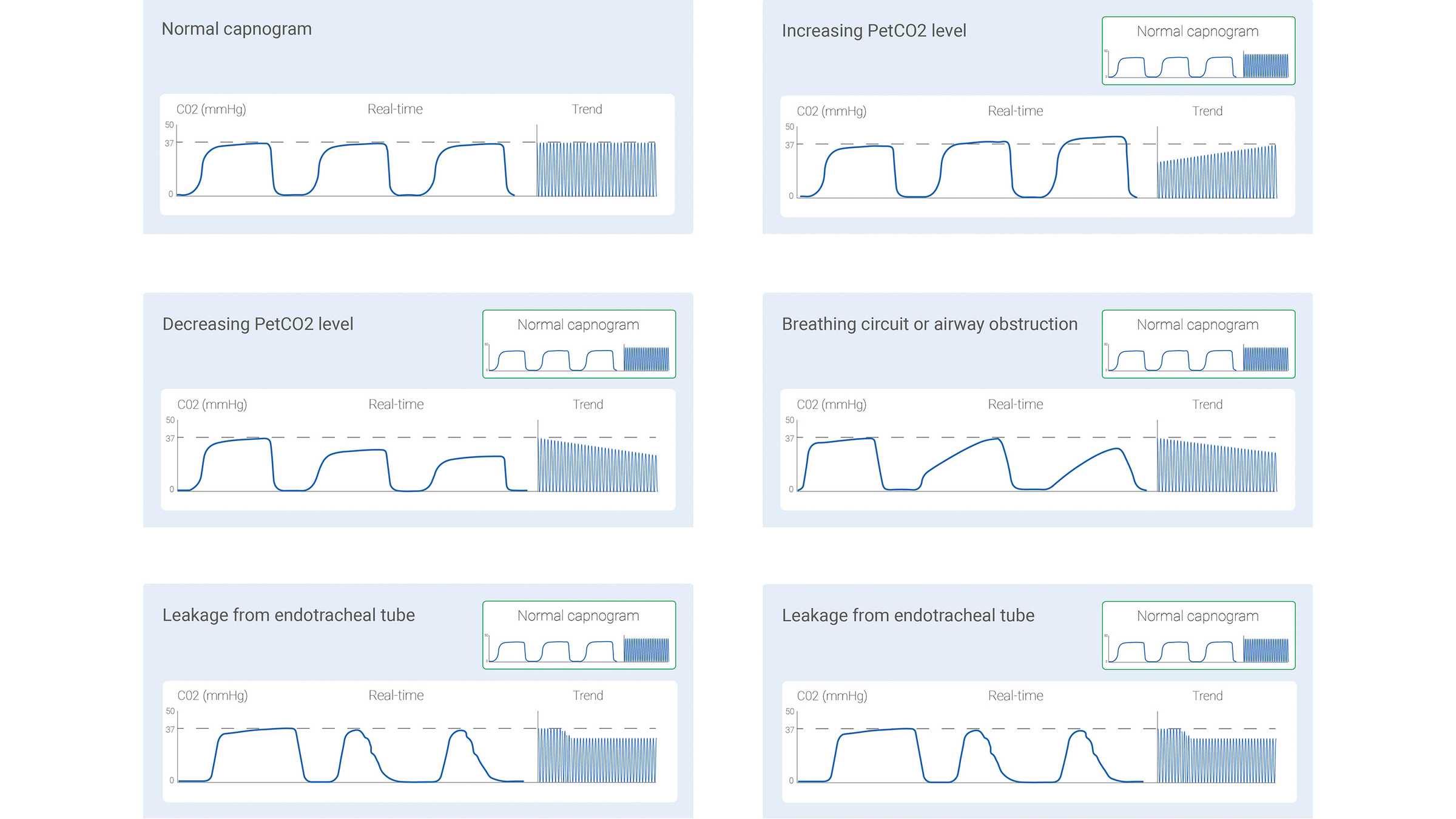
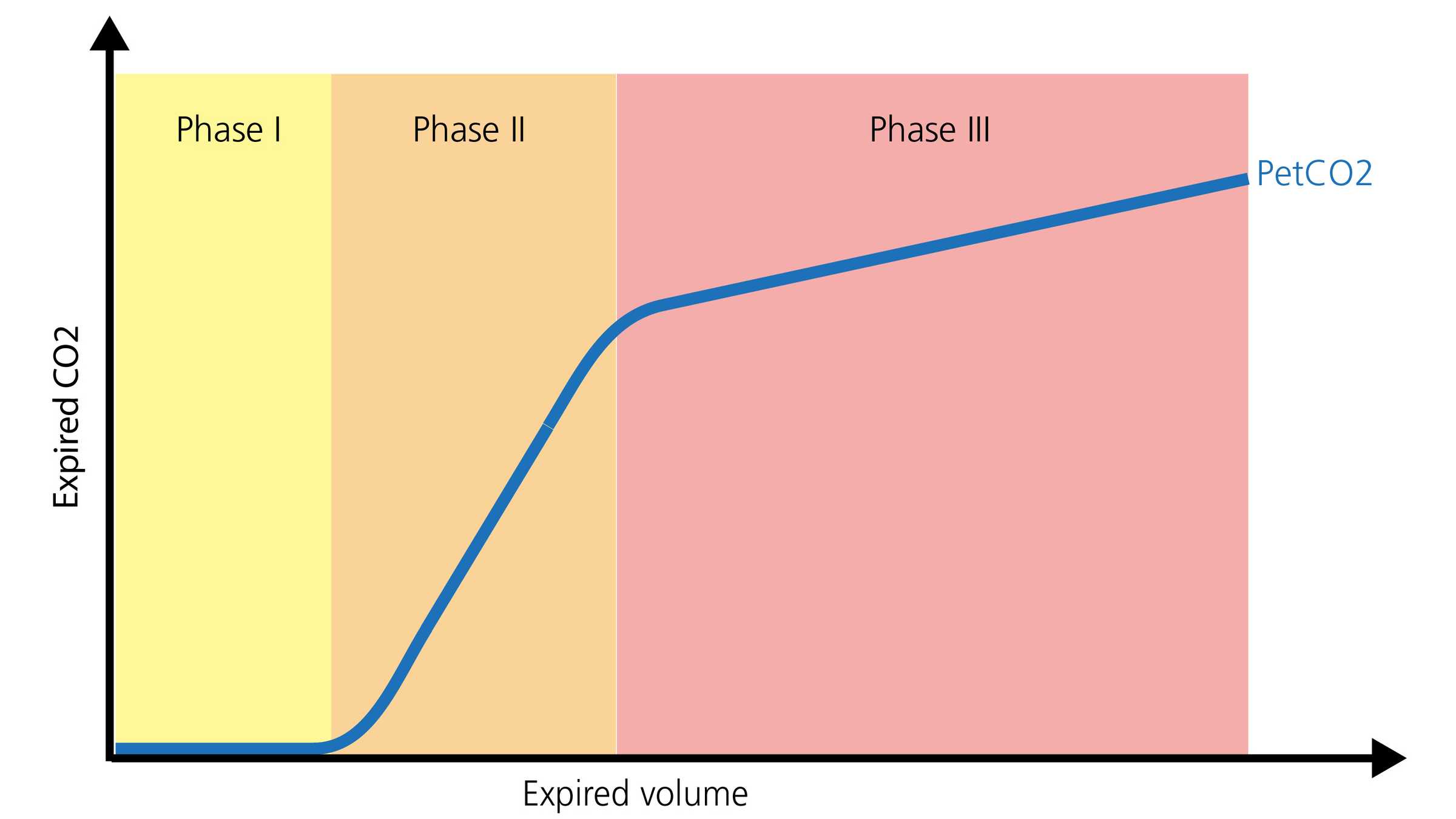
Измеренный сигнал датчика CO2 может быть записан либо как функция времени (капнография, контролируемая по времени), либо как функция выдыхаемого объема (волюметрическая капнография). Объем информации, которую можно получить при использовании этих двух разных типов капнографии, значительно отличается. В литературе описаны определенные закономерности капнограммы, контролируемой по времени, которые считаются типичными для конкретных клинических ситуаций. Некоторые из общих закономерностей показаны на рисунке 1 ниже.
Однако капнография, контролируемая по времени, также имеет ограничения. Он не может обеспечить точную оценку состояния вентиляции и перфузии легких, а также не может использоваться для оценки компонента физиологического мертвого пространства. Волюметрическая капнография не так проста и удобна, как капнография, контролируемая по времени, однако ее преимущество заключается в значительно большем объеме информации.
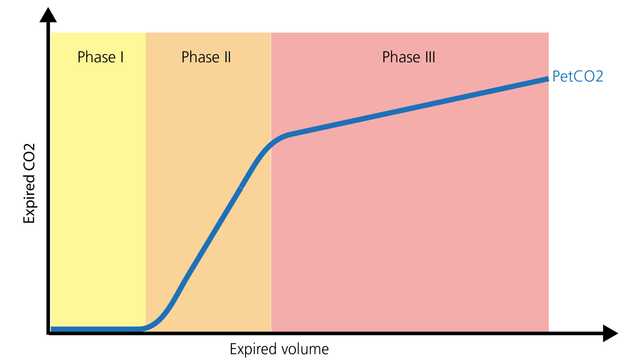
Нормальная форма волюметрической капнограммы состоит из трех фаз. Важно помнить, что капнограмма отражает выдох.
С помощью капнографии, как контролируемой по времени, так и волюметрической, можно получить ценную информацию для оптимизации мониторинга и лечения пациентов, которым требуется транспортировка в пределах больницы или в другие больницы. Ее можно безопасно использовать с эндотрахеальными трубками, трахеостомическими трубками и многими надгортанными воздуховодами при наличии необходимого уплотнения. Расположение и проходимость дыхательных путей, мониторинг вентиляции и состояние перфузии – все это области, в которых PetCO2 предоставляет важную информацию. Еще одним значимым параметром является объем углекислого газа, выводимого за минуту (V’CO2), который позволяет медицинскому персоналу оценивать эффективность перфузии и реанимационных мероприятий (
У пациентов отделения интенсивной терапии капнография может продолжать мониторинг расположения и проходимости дыхательных путей с использованием различных дополнительных средств. Соотношение мертвого пространства и дыхательного объема (VD/Vt) является важным показателем капнографии. Увеличение соотношения VD/Vt может означать потенциальное увеличение смертности в зависимости от уровня увеличения (
Во всех аппаратах ИВЛ Hamilton Medical доступна волюметрическая капнография (
Узнайте, как читать волюметрические капнограммы, каковы их преимущества и где применять полученные данные. Книга также содержит тест для самопроверки.