


作者: Giorgio A. Iotti, Jean-Pierre Revelly
日期: 30.08.2023
A recent paper on the practical assessment of the risk of ventilator-induced lung injury (VILI) from mechanical power (MP) brings several important and interesting observations.
The paper by John Marini and co-authors (
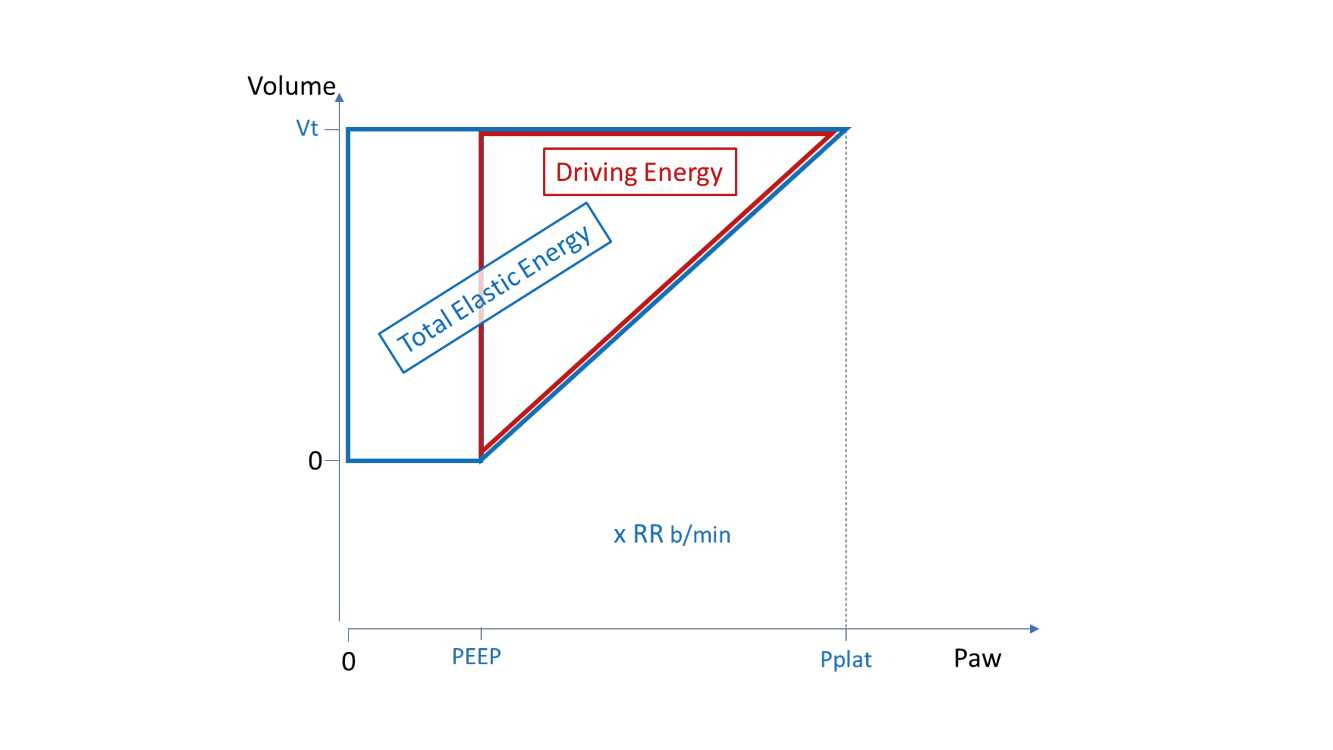
As already discussed in a previous newsletter, MP corresponds to the energy associated with each inflation multiplied by the respiratory rate per minute. In turn, the total energy corresponding to each breath is divided up into resistive energy and elastic energy. Here, the authors leave out the resistive energy and focus on the elastic one, bearing in mind that only the elastic energy correlates strongly with the stretch and strain that have the potential to damage the lungs under dynamic conditions. Focusing only on the elastic energy greatly simplifies the use of MP for assessing the risk of VILI, because (in contrast to Total MP) Elastic MP is largely independent from the ventilation mode (volume- or pressure-controlled) and can be calculated from simple measurements during passive ventilation. Neglecting the resistive energy might also mark the end of the scientific debate about the method for evaluating Total MP (
Subsequently, two different kinds of elastic energy are considered (see Figure 1): the “driving energy” associated with the driving pressure (DP) applied above PEEP to develop the tidal volume (VT), and the “total elastic energy” associated with the gauge pressure above atmospheric pressure (i.e., the plateau pressure: Pplat = DP + PEEP) applied to develop the VT. Taking both these types of elastic energy into account should put to rest the scientific debate about whether PEEP should be considered for the calculation of MP (
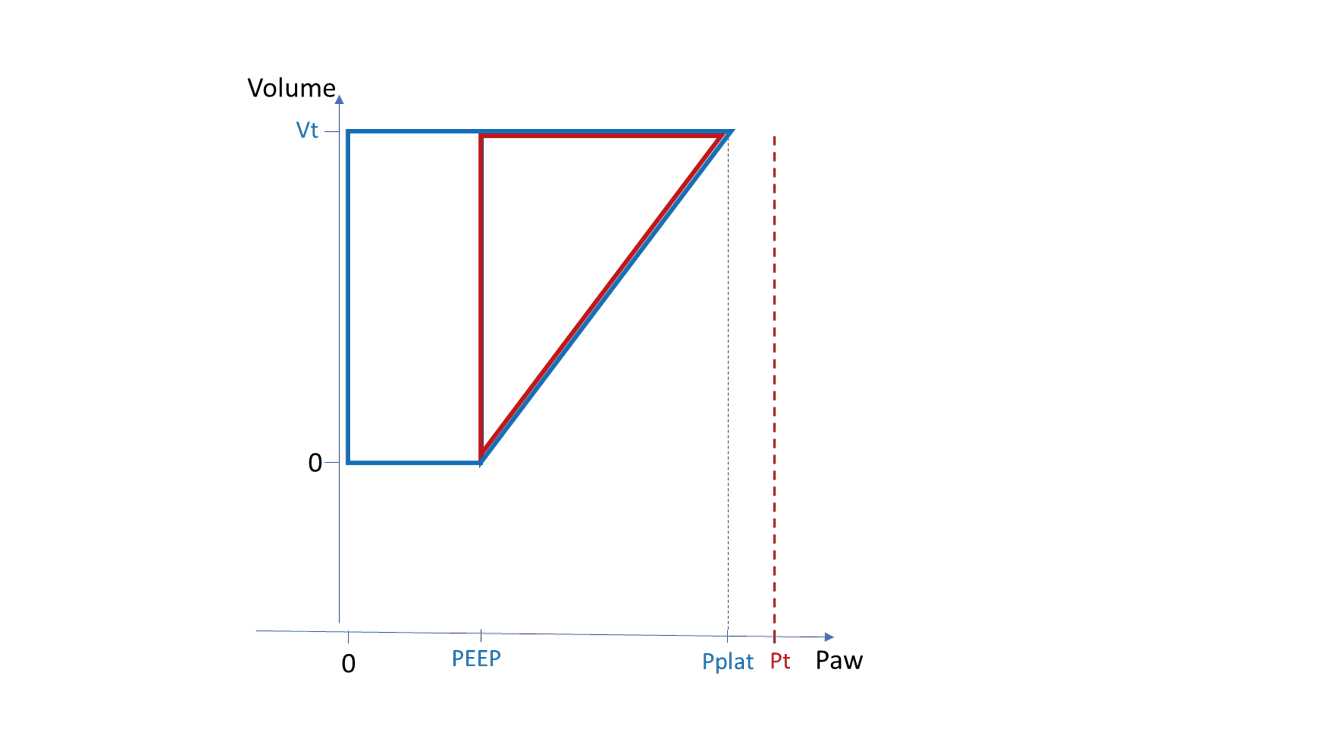
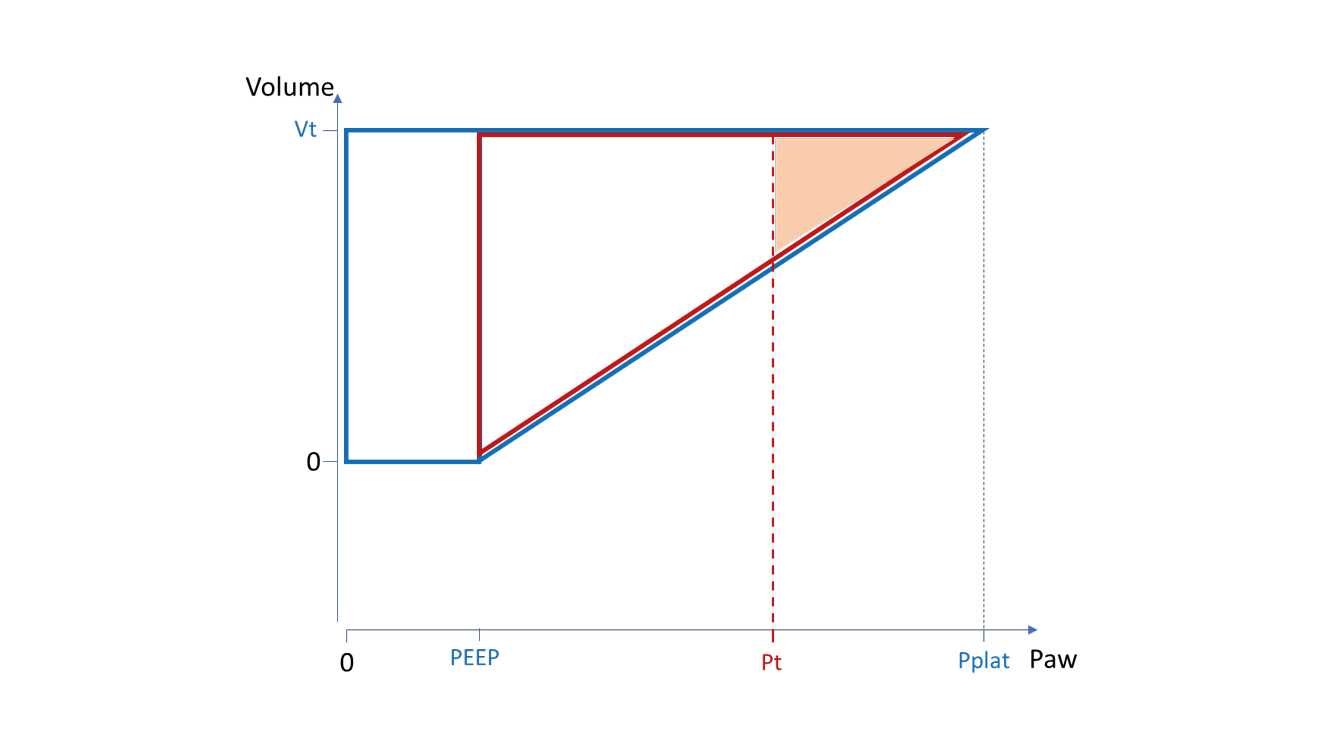
Finally, Marini recommends considering - for both DP and Pplat - a threshold pressure (Pt) for mechanical damage to the lungs. In the diagrams below, Figure 2 represents a case in which ventilation is managed with elastic pressures below the Pt and the theoretical risk of VILI is therefore zero. In this case a high respiratory rate, although associated with a substantial Driving MP and Total Elastic MP, should not increase the risk of VILI. In Figure 3, the elastic pressures at the top of inspiration marginally exceed the Pt; therefore, the associated mild risk of VILI is amplified by an increase in respiratory rate. The results are much worse in the example represented in Figure 4 where a high respiratory rate will considerably contribute to the risk of VILI.





Although the PEEP level has a direct effect on total elastic energy per breath, and hence on Total Elastic MP, the choice of PEEP is normally based on other criteria than the resulting MP (such as gas exchange, hemodynamics, etc.). In contrast, the breaths developed on top of PEEP should be set to avoid them exceeding Pt. For Pt, a rough choice can be made by combining the two numbers that are currently recommended for lung protection: maximum DP = 15 cmH2O and maximum Pplat = 30 cmH2O.
To satisfy both criteria, this means that for a PEEP of 12 cmH2O, for example, Pplat should not exceed 12 + 15 = 27 cmH2O. If PEEP is 15, the maximum Pplat should be 15 + 15 = 30 cmH2O; while if PEEP is 18 and the maximum Pplat should still not exceed 30 cmH2O, then DP should not be higher than 30 – 18 = 12 cmH2O. Under these conditions, the respiratory rate can theoretically be increased as much as needed to control arterial PCO2 and pH, without any additional risk of lung damage.
However, if we are forced for any reason to ventilate with elastic pressures that exceed the Pt, it may not be so easy to find the ventilatory pattern that is of minimal detriment to the lungs and of maximal efficiency for CO2 elimination at the same time. In principle, the automatic selection of respiratory rate and VT made by ASV and INTELLiVENT-ASV might be very helpful for that purpose, while the calculation of Total Elastic MP and Driving MP should enable an assessment of the risk associated with the ventilation in progress.
The authors do not ignore the practical limits of their model. The use of Pt based on maximum DP = 15 cmH2O and maximum Pplat = 30 cmH2O is just a general approach; for individual patients or for different lung zones of their respiratory system, a different Pt may be more appropriate. In particular, a high pleural pressure (as in the case of a stiff chest or heavy chest) should have a protective effect on the lungs and thus allow a higher Pt than normal. In addition, the gravitational pleural pressure gradients should be taken into account. This means that in supine position, the Pt should be lower in the non-dependent lung regions, but higher in the dependent regions protected by a higher pleural pressure. The effects of gravity on Pt should be much less pronounced in prone position.
We sincerely thank John Marini for his ongoing contribution to a better understanding of mechanical ventilation and respiratory mechanics, and for sharing his brilliant insights with the intensive care community.