




人机不同步是指病人与呼吸机的吸气和呼气时间之间不匹配。检测不同步的一个常用方法是通过分析呼吸机波形。不同步有不同的类型,每种类型都有一组可以目视识别的特征。训练有素的眼睛可以通过分析流量或压力波形图来检测人机不同步 (
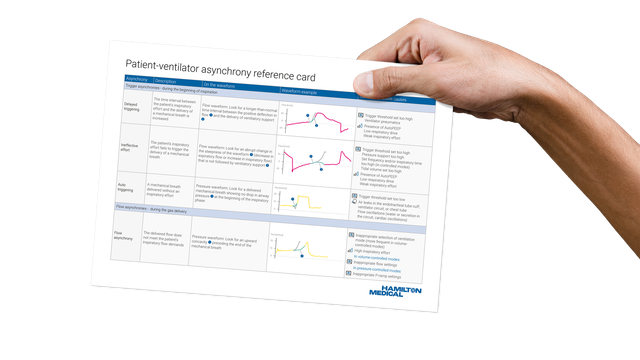
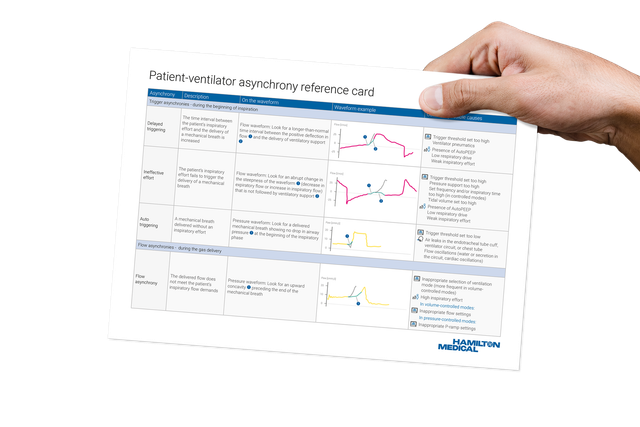
为帮助您识别每次不同步的迹象特征,我们创建了一种两页式参考卡(也称为“备忘单”),您可以在下方下载该参考卡。
您可通过它快速了解:
7 种主要类型的不同步
压力或流量波形上的查找信息指征
突出显示最易识别特征的波形的可视示例
不同类型不同步的常见可能原因
不要错过提高您的机械通气知识水平的机会。