作者: David Grooms
日期: 08.07.2019
The most common causes are:
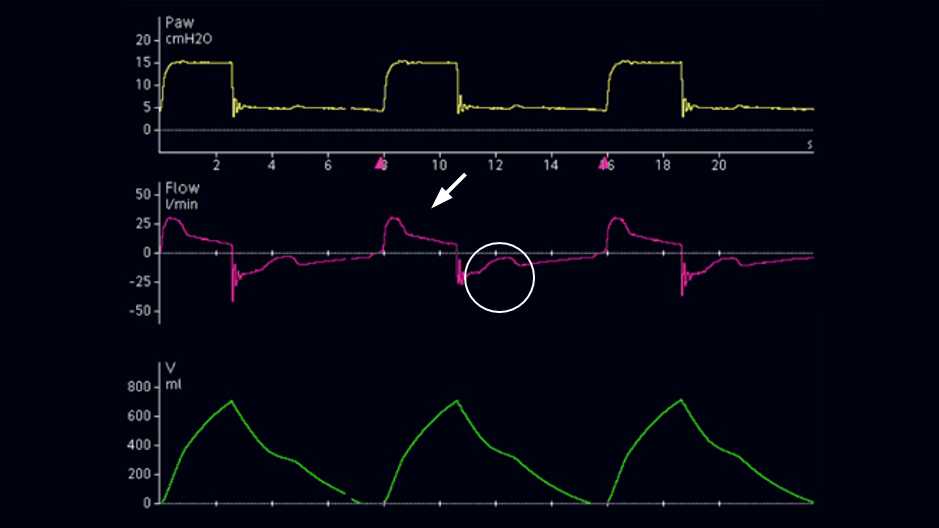
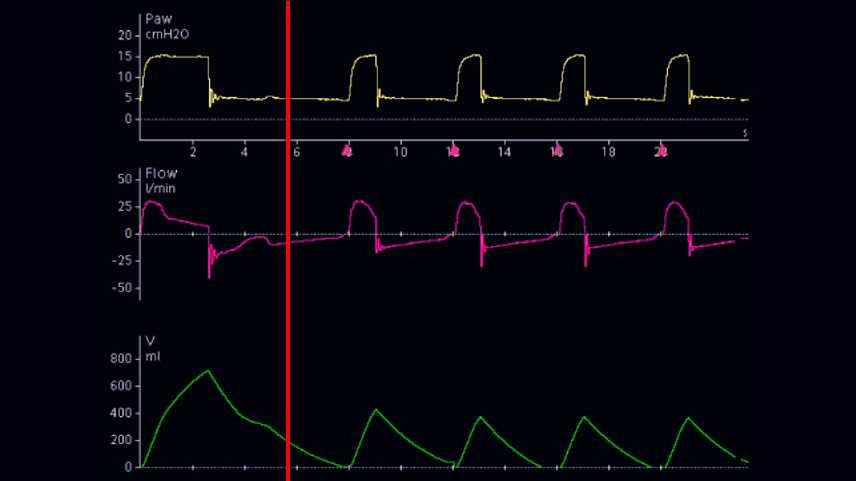
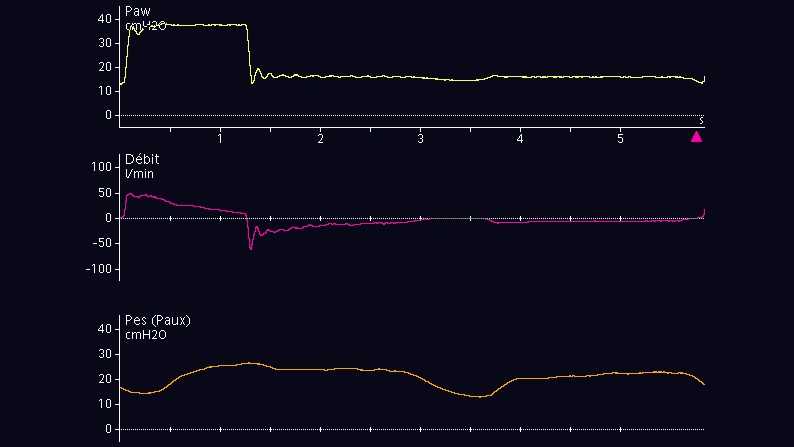
Several waveform characteristics can assist in the diagnosis (see Figure 1):

The most practical adjustments that can be made on the ventilator to reduce ineffective efforts are as follows: