



Author: Jean-Michel Arnal、サント・ミュス病院(フランス、トゥーロン)
Date of first publication: 18.09.2025
Last change: 10.06.2026
Typo correction静的ドライビングプレッシャーをベッドサイドで体系的にモニタリングする必要がありますが、どのように測定すればよいのでしょうか?
補助換気モードを使用している人工呼吸器装着患者において、静的ドライビングプレッシャー(∆PSTAT)は単独でICU生存率と関連してしています(
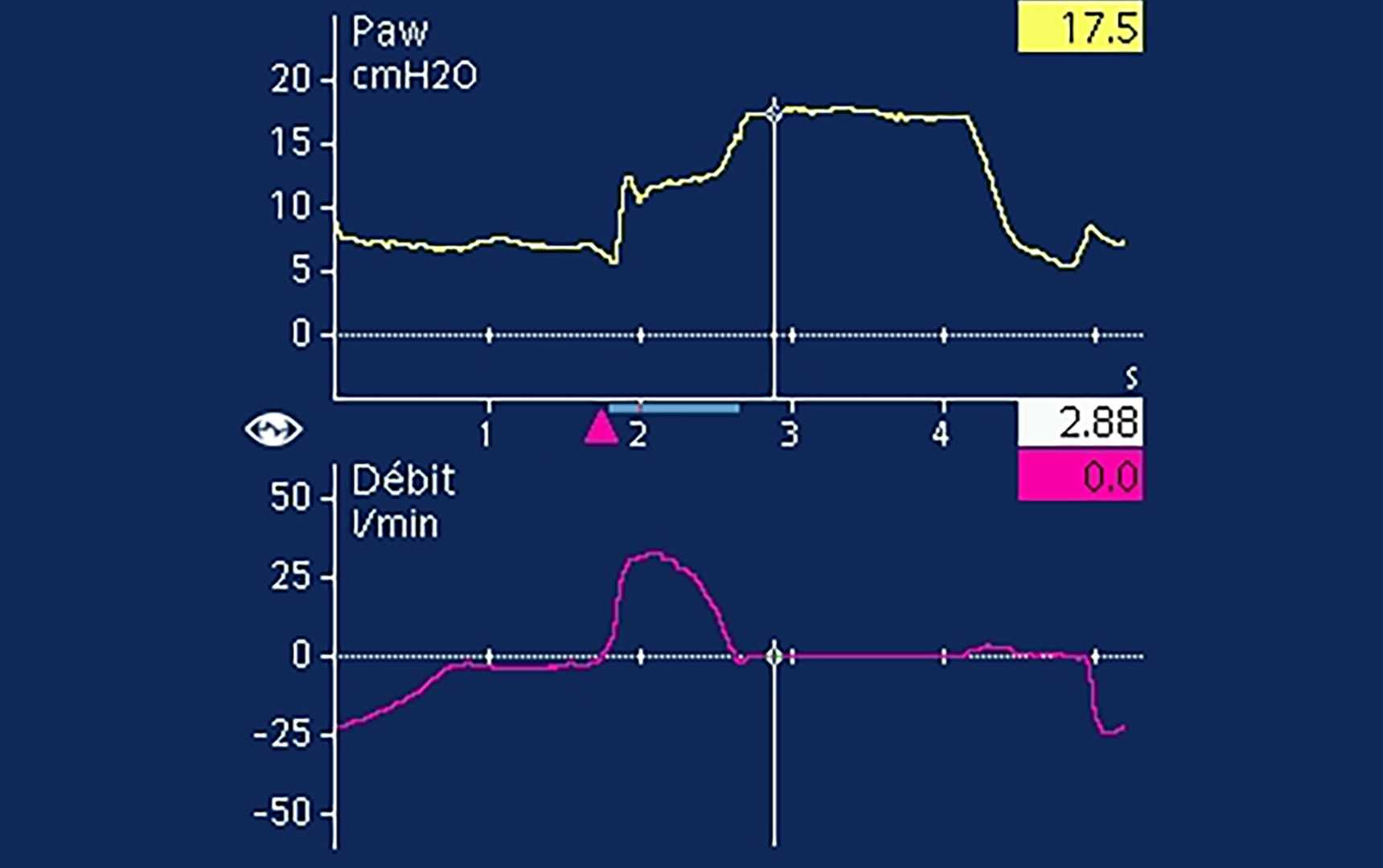
補助換気におけるPPLATの測定には吸気終末閉塞法を使用しますが(

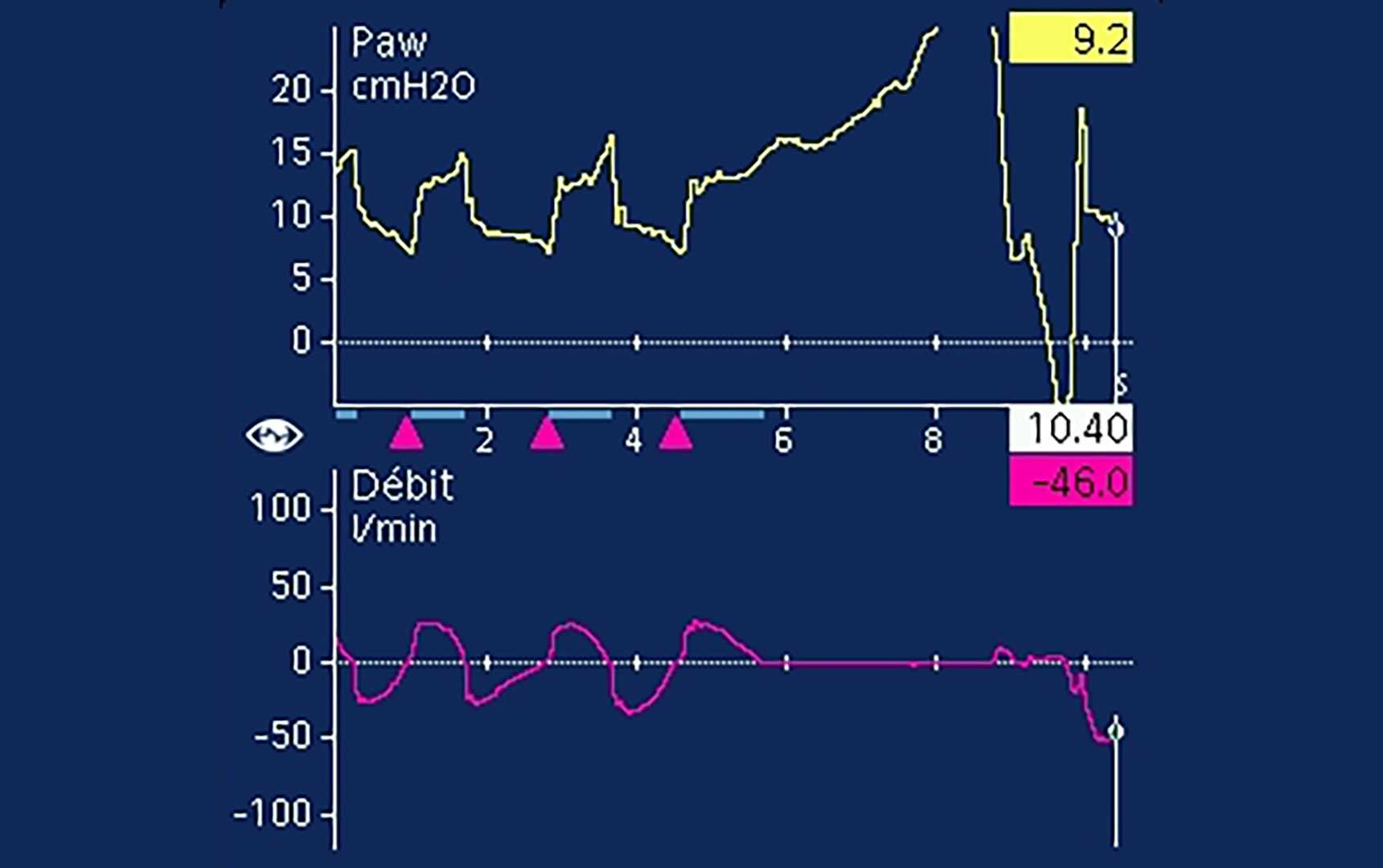

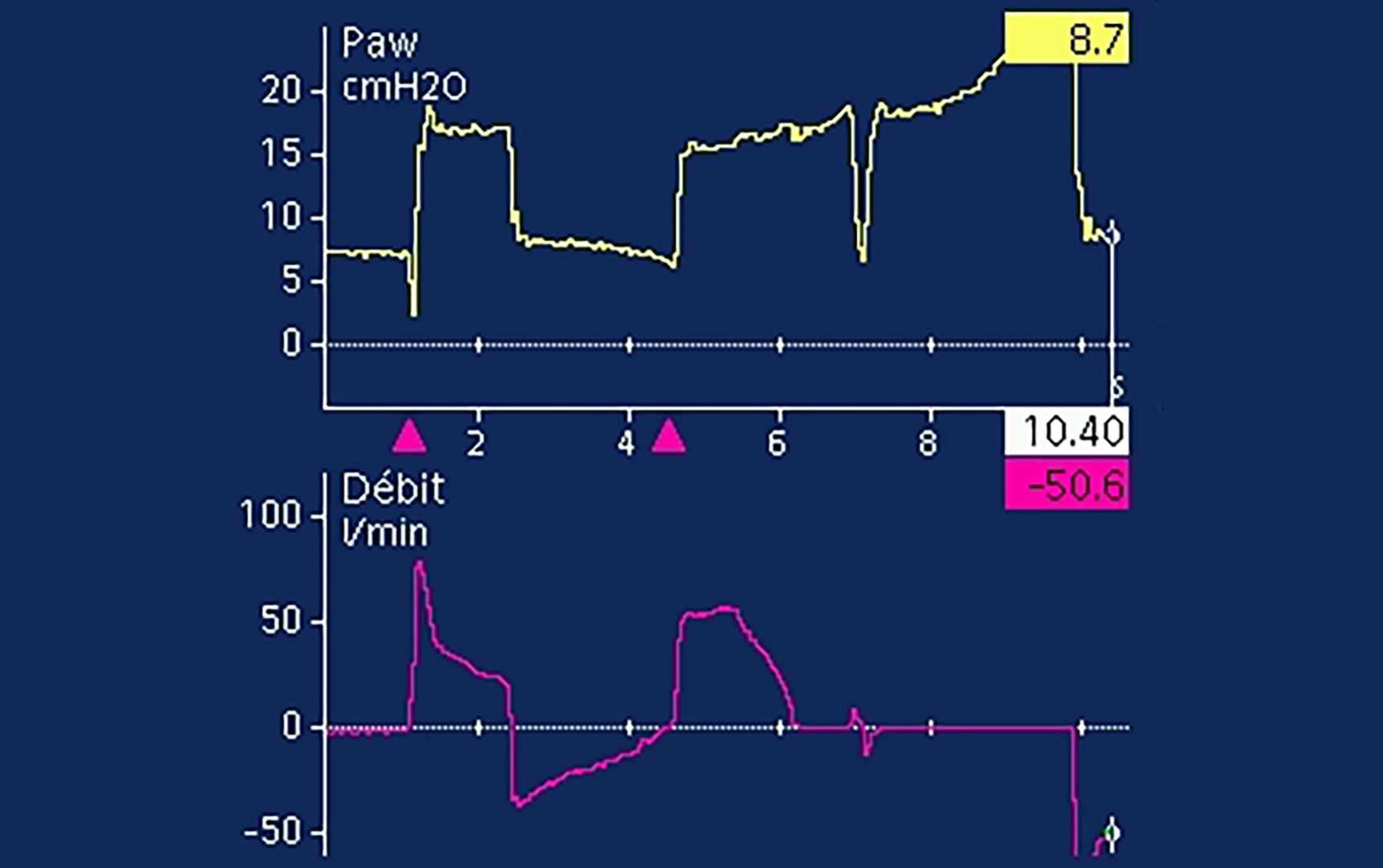
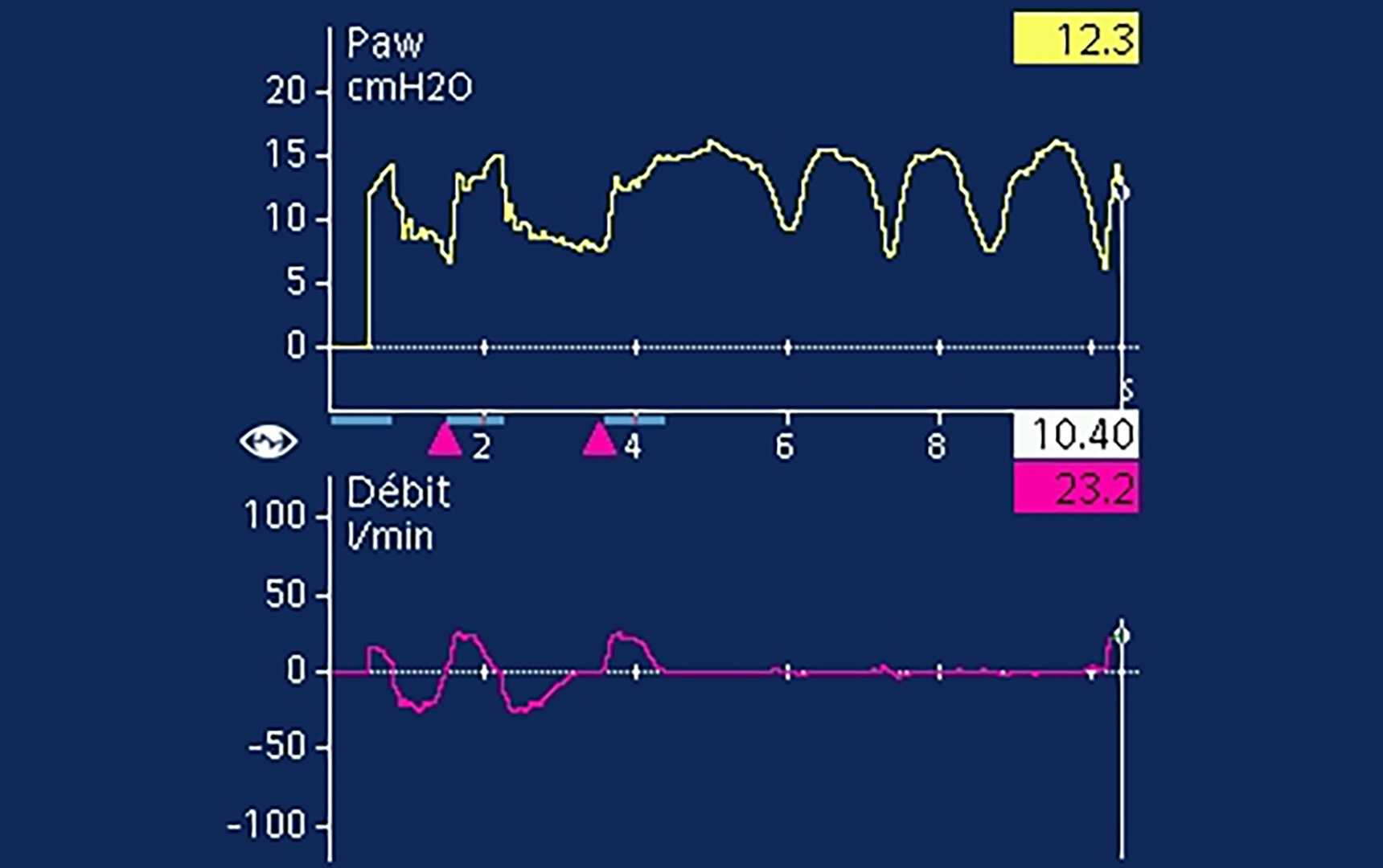
明白なプラトーが視認できる場合でも、呼気筋の活動が存在することは少なくありません(
