


Author: Jean-Pierre Revelly、Giorgio Iotti
Date of first publication: 03.04.2023
この記事では、メカニカルパワーを構成する要素、臨床状況におけるその関連性、およびモニタリングパラメータとしてのメカニカルパワーの使い方について詳しく見ていきます。
この議論の範囲はコントロール換気の吸気フェーズ中のメカニカルパワー(MP)に限定されており、患者の呼吸努力はないと仮定しています。
物理学では、
人工呼吸では、吸気中に人工呼吸器から呼吸器系に伝達されるパワーは、人工呼吸器誘発肺傷害(VILI)を引き起こす可能性のある要素を組み合わせた統合変数です(
一定流量の適応調節強制換気(CMV)において、MPは呼吸あたりの仕事量(W)×呼吸回数(RR)で表すことができます(図1)(
ここで、

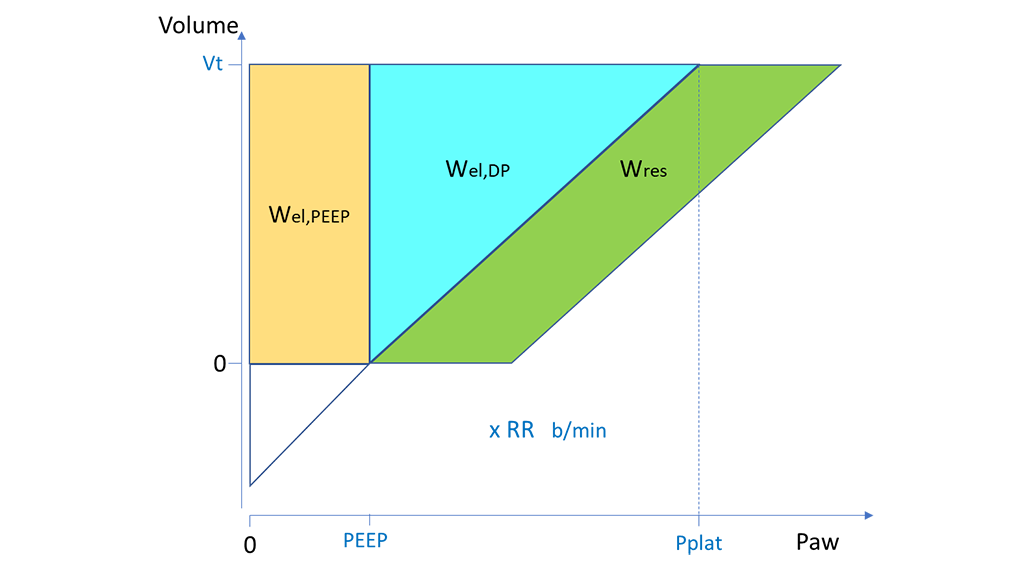
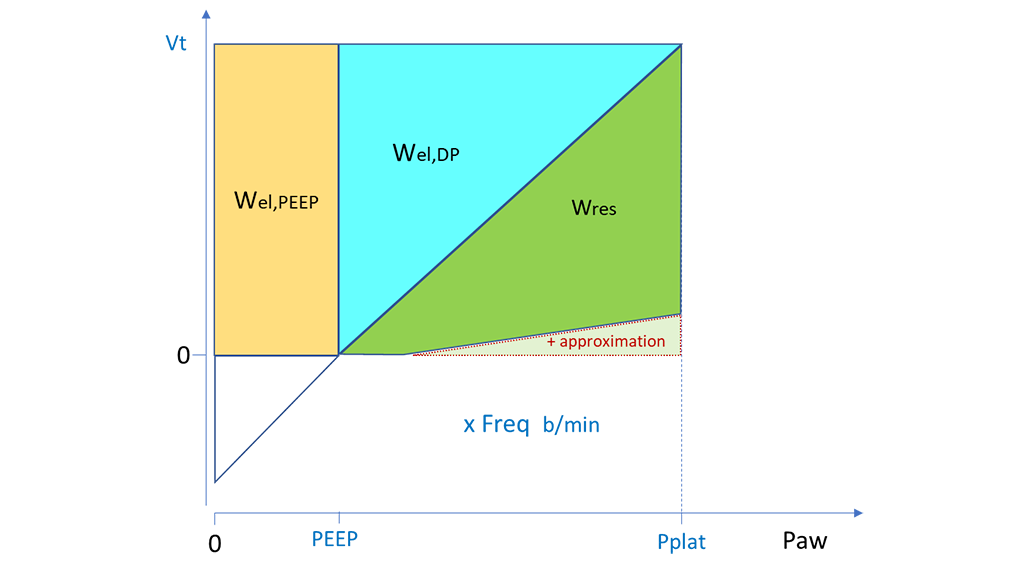
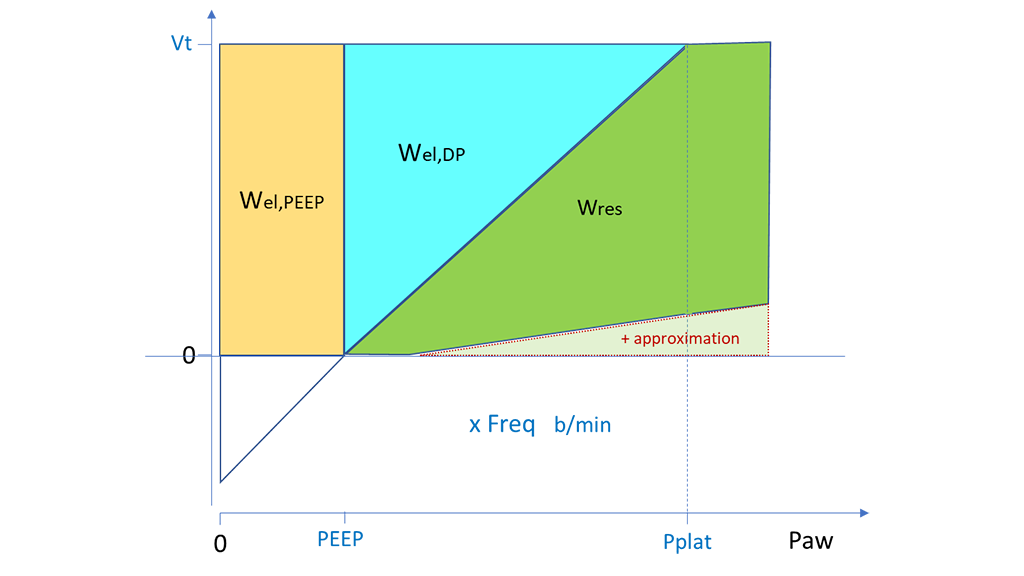
プレッシャーコントロール換気(PCV)では、Vt、PEEP、DPからのWel,PEEPとWel,DPの計算については同様のアプローチをとることができます。Wresについては、Ppeak - PEEPを底辺、Vtを高さとする四角形の面積を計算し、そこからWel,DPに対応する三角形を減算することで、概算できます。このWresの計算は、PpeakがPplatと等しい場合(図2)またはPplatより高い場合(図3)に同じように適用できます。前者は吸気終末流量がゼロである場合、後者は正である場合をそれぞれ示します。この計算方法は概算なので、どちらの場合もWres(したがって、人工呼吸器の真の総仕事量)は若干過大評価されます(


これまでかなりの数の研究者が、ARDSを持つICU患者(
これらの分析の結果は次のとおりでした。
全体的に見て、これらの後ろ向き研究は、臨床転帰不良がVILIにある程度関連していると仮定した場合、過度のMPは避けるべきであることを示唆しています。
MPの計算方法を適切に解釈するため、公表された研究でMPがどのように計算されているかを慎重に読む必要があります。MPのどの要素が含まれている、または除外されているかは、使用可能なデータによって異なる場合があります。また、異なる患者を比較する最適な手順についても議論が続いています。患者の体格(予想体重)、コンプライアンス、または呼気終末肺容量について正規化することが提案されています。
ただし、一般的に言えば、MP計算の標準化されたアプローチはまだ確立されておらず、推定MPに対する広く受け入れられた安全値もありません。
人工呼吸器の設定の個別の変更は、換気メカニクスの他の変数に複雑な影響を与えます。MPの概念は、「すべての換気変数がVILIに対して直線的な関係を持ち、VILIに同じように寄与する」という暗黙の前提に基づいています。しかし、これは明らかに事実とは異なります。たとえば、PEEPはVILIに対して曲線的な(J字型の)関係を持ちます(
一連の未解決の問題が残ってはいるものの、総MPとその要素をモニタリングすることは、個々の患者の漸進的変化や換気設定の変更に対する反応を評価するうえで有用である可能性があります。MPは、他のいくつかの項目とともに、臨床判断や意思決定を行う際の新たな検討材料になる可能性があります。さらに、MPのモニタリングは、MPとVILIの関係について調べる前向き研究で質の高いデータを収集するために大いに役立ちます。
これまでさまざまな研究者が、換気の最も有害な要素を特定しようと試みてきました。管理下試験に登録された4500例のARDS患者の換気データを集計したある後ろ向き研究で、MP、Vt、RR、DPの28日死亡率に対する関係が多変数モデルを使用して評価されました(
この後ろ向き研究では、予想どおり、全体的MPが死亡率と相関していました。MPの各要素については、弾性動的要素(MPel,DP、すなわちWel,DPに依存するMP)だけが統計的有意性を示し、PEEPまたは抵抗に依存する要素は統計的に有意ではありませんでした。MPel,DPはとりわけ、CMVとPCVのどちらにおいても、ベッドサイドで計算しやすいという特徴があります。
さらに、DPとRRから計算される次の指標にも、死亡率について同等の予測性がありました。
著者らは、「メカニカルパワーはARDS患者の死亡率と関連性があったが、∆PとRRも同様に有益であり、ベッドサイドで評価しやすい。これらの変数に基づく換気戦略によって転帰が改善されるかどうかを無作為化対照試験で調べる必要がある」と結論付けています(