




Author: Giorgio Iotti、Caroline Brown
Date of first publication: 29.04.2025
人工呼吸器のモニタリング値からリクルートメント対拡張比を計算する方法。
リクルートメント対拡張比(R/I)は、臨床医がベッドサイドで患者のリクルータビリティを評価し、その結果に応じてPEEPを設定する手段を提供します。Chenらが説明している単一呼吸法 (
以下の手順では、HAMILTON-C6人工呼吸器でこれを行う方法を示します。
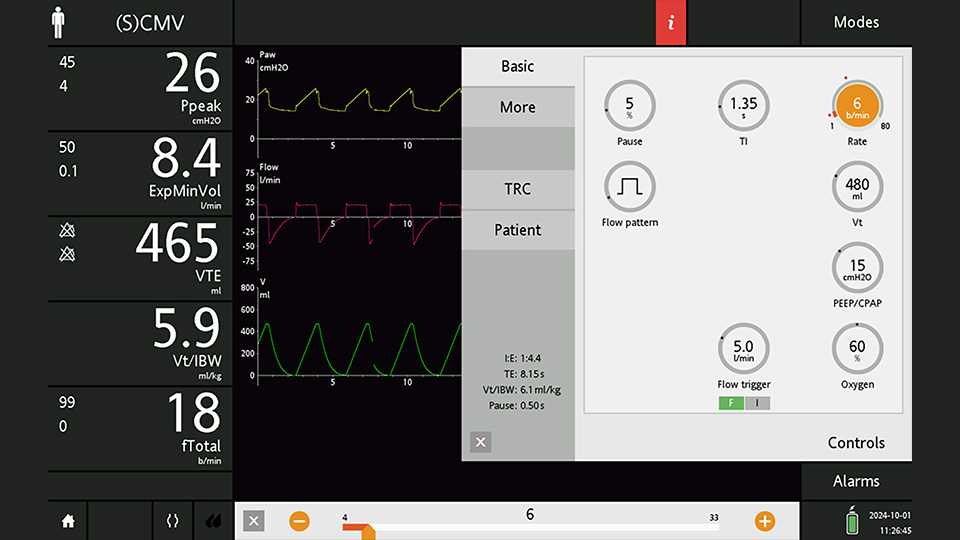
PEEPを15 cmH2Oに設定した(S)CMVモードで患者を30分換気します(図1を参照)。吸気ポーズは少なくとも5%に設定します。画面を静止する前に波形の該当する部分が流れてしまわないように、時間スケールを30秒に設定することを推奨します。



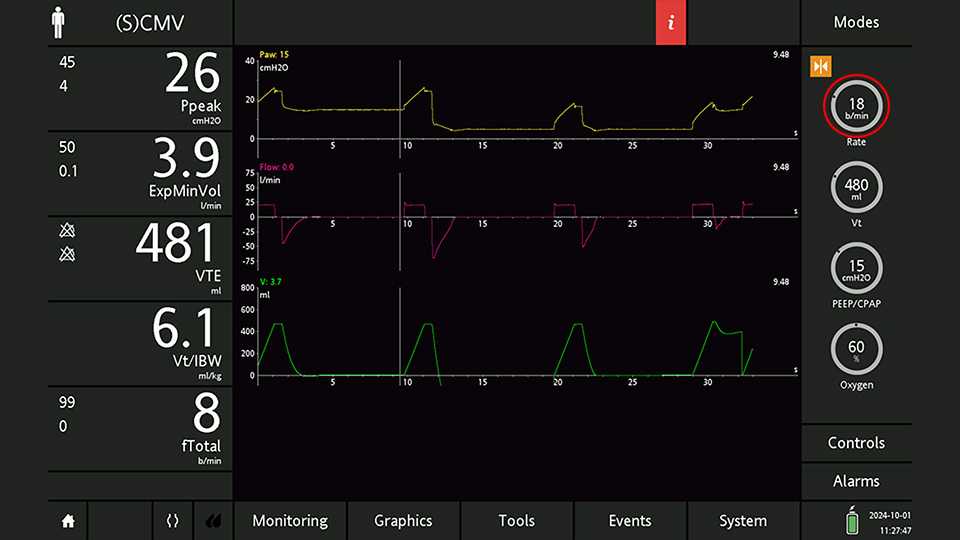
カーソルを高い方のPEEPレベルでの最後の呼気の終わりに移動します(図5を参照)。

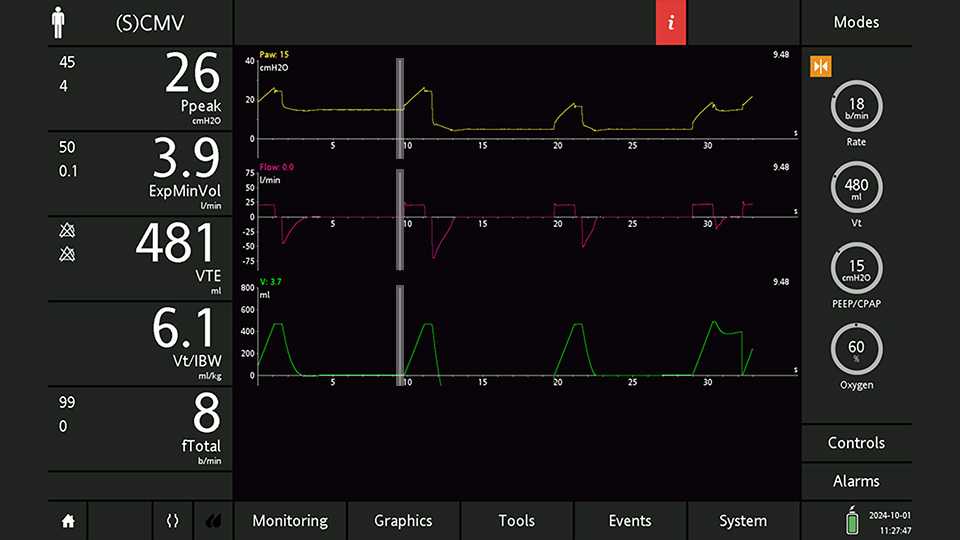
カーソルを低い方のPEEPレベルでの最初の呼気の終わりに移動します(図6を参照)。ここで、PEEP,lowの実際の値と、ベースラインに対する呼気終末量(End-exp Vol。波形上には表示されませんが、カーソルによって読み取ることができます)を測定します。収縮とデリクルートメントによる追加分の呼気VT(VTe,plus)は、End-exp Volの正負を反転させた数値です。
これでPEEPの差を計算できます。

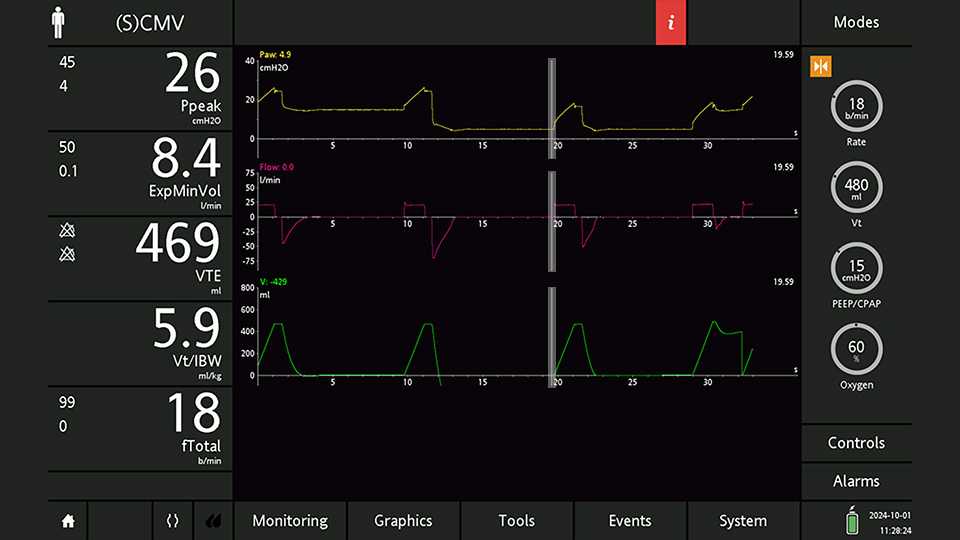
カーソルを低い方のPEEPレベルでの最初の吸気プラトーの終わりに移動します(図7を参照)。ここで、プラトー圧(Pplat,low)と吸気VT(VTi,low)を測定します。
これで、低い方のPEEPレベルでのドライビングプレッシャーとコンプライアンスを計算できます。
ステップ1、2、3でカーソル測定値をメモした後、忘れずにPEEP設定を確認してください。R/I比の測定に必要なのは、PEEPレベルを下げた状態での呼吸1回分だけです。PEEPレベルを下げた状態のまま長時間換気を続けると、肺胞が広範囲に虚脱し、結果的にガス交換が著しく悪化する可能性があります。


メモした値を使用して、上記のステップで設定したPEEPの変化に伴う肺胞拡張によるボリュームの変化(Vinflated)と肺胞リクルートメントによるボリュームの変化(Vrecruited)を計算できます。
これら2つの値からリクルートメント対拡張比を計算します。
R/I比が0.3~0.4より低い場合は、リクルータビリティが低いことを示します。ここに示す例の場合は、PEEP設定を低くする(5~8 cmH2Oにする)のがより適しています。それに対して、R/I比が0.6~0.7より高い場合は、リクルータビリティが高いことを示します。この場合は、PEEPレベルを少なくとも12 cmH2Oに設定することが推奨されています。R/I比が0.5前後の場合は、中間のPEEPレベルが推奨されます(
