




Autore: Giorgio Iotti, Caroline Brown
Data: 29.04.2025
How to determine the recruitment-to-inflation ratio from monitoring values on your ventilator.
The recruitment-to-inflation ratio (R/I) offers clinicians a bedside means of assessing a patient’s recruitability so PEEP can be set accordingly. Using the single-breath technique as described by Chen et al. (
In the following steps we show you how to perform the technique on a HAMILTON-C6 ventilator.
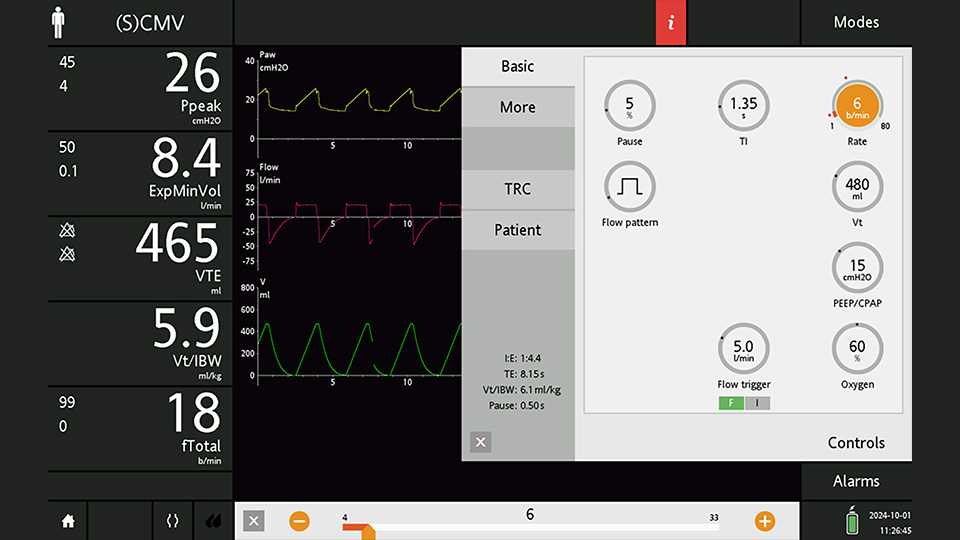
The patient should be ventilated in (S)CMV mode with a PEEP of 15 cmH2O for 30 minutes (see Figure 1). Pause for inspiration should be set at the minimum of 5%. We recommend using a time scale of 30 seconds to ensure the relevant part of the curves do not disappear before the screen freezes.



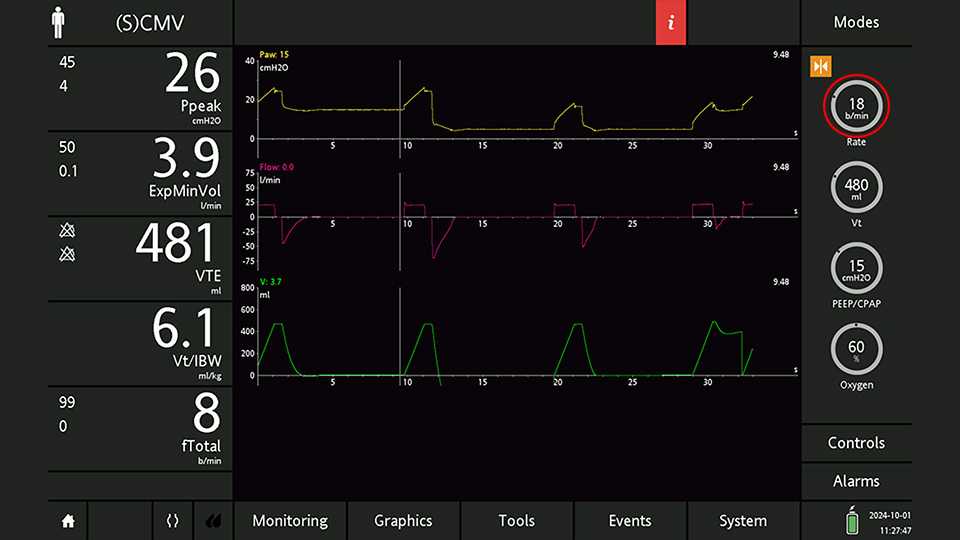
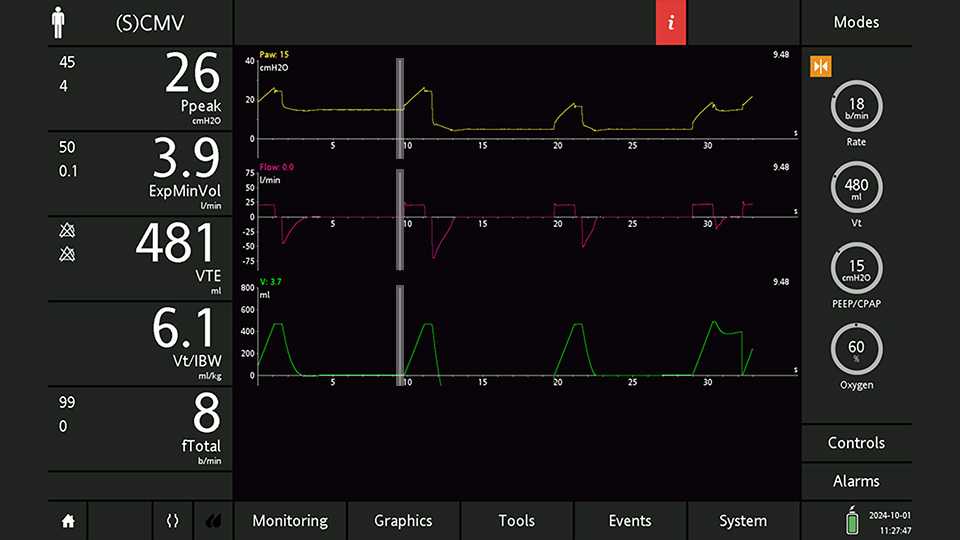
Place the cursor at the end of the last expiration at the higher PEEP level (see Figure 5).

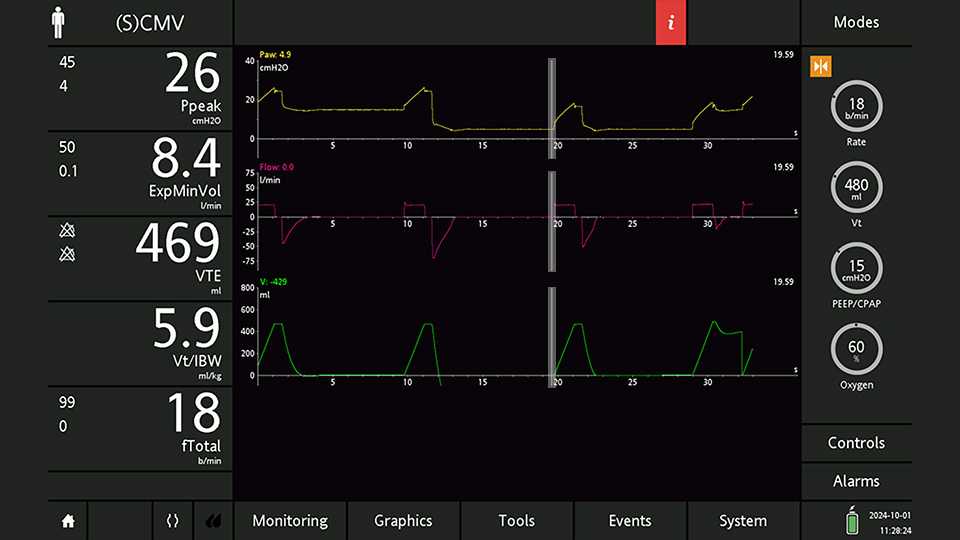
Move the cursor to the end of the first expiration at the lower PEEP level (see Figure 6). Here you measure the actual value of PEEP,low and the end-expiratory volume relative to the baseline (End-exp Vol, not visible on the curve but readable by the cursor). The additional expiratory VT due to deflation and derecruitment (VTe,plus) is the opposite of End-exp Vol.
Now you can calculate the difference in PEEP:

Move the cursor to the end of the first inspiratory plateau at the lower PEEP level (see Figure 7). Here you measure the plateau pressure (Pplat,low) and the inspiratory VT (VTi,low).
Now you can calculate driving pressure and compliance at the lower PEEP level:
After taking note of the cursor measurements as described for steps 1, 2, and 3, do not forget to check the PEEP setting. The R/I ratio measurement requires just one breath at the lower PEEP level. Prolonging ventilation at the lower PEEP level may result in extensive alveolar collapse with severe worsening of the gas exchanges as a consequence.


With the values you have made note of, you can now calculate, for the PEEP change you have explored, the volume change just due to alveolar inflation (Vinflated) and the change due to alveolar recruitment (Vrecruited).
These two values give you the recruitment-to-inflation ratio.
R/I values lower than 0.3 – 0.4 indicate low recruitability. As is the case here, a low PEEP setting (of between 5 and 8 cmH2O) may be the more appropriate choice. On the other hand, a PEEP level of at least 12 cmH2O has been suggested when R/I values higher than 0.6 – 0.7 indicate high recruitability. Intermediate PEEP levels are suggested when R/I is found to be around 0.5 (
