



Autor: Hamilton Medical, with Dr. Mario Rugna, U.S.L. Toscana Centro
Data da primeira publicação: 17.07.2026
Hamilton Medical explores the evolution of emergency respiratory care with Dr. Mario Rugna, Medical Director of Extra-Hospital Medical Education at the U.S.L. Toscana Centro.
A blaring siren sounds, the clock is ticking, and a life hangs in the balance. A bag, valve, and mask (BVM) functioned as the principal device for immediate respiratory support (
To better understand this evolution and what the future of prehospital ventilation could look like, Hamilton Medical sat down with Dr. Mario Rugna to gain insights and assess the impacts of moving mechanical ventilation into the treatment algorithm.
Dr. Rugna is the Medical Director of Extra-Hospital Medical Education at the U.S.L. Toscana Centro in Florence, Italy, overseeing prehospital services across 13 hospitals and 1.5 million residents. He is also an emergency flight physician for Tuscany’s Regional Helicopter EMS. With a background in ER medicine, Dr. Rugna transitioned to prehospital care and now leads a team of over 300 providers. He has played a central role in training EMS personnel and is a strong advocate for integrating mechanical ventilation into prehospital emergency care.
Evolution often begins by combining classic, manual interventions with more modern, mechanical solutions. The prehospital care space is no different, as limitations of the traditional BVM (
Today’s care teams are generally aware of the benefits of mechanical ventilation and the challenges associated with the manual nature of the BVM. Known limitations include maintaining an adequate minute volume (consistent tidal volumes, rate, breath phase/I:E ratio or i-Time) and optimal airway pressures, correct measurement and maintenance of appropriate PEEP, leak detection, and operator fatigue. Although mechanical ventilation is able to counter these issues, it remains underutilized in practice.
Transport care experts like Dr. Mario Rugna believe the slow transition from the BVM is due to training barriers and adoption dynamics unique to prehospital and emergency medicine, despite widespread clinical evidence (
Clinicians rely on a bag in their hands, “because we are humans,” explains Dr. Rugna. “In the moment when you are out in the street with a young patient that is in cardiac arrest, you don’t think about the volume that you inflate, and you don’t think about the respiratory rate." For many, the BVM is a literal metaphor for those ‘touch-and-go' scenarios that highlight the gap between current manual practices and greater use of mechanical ventilation.

In Dr. Rugna’s experience, the underutilization of mechanical ventilation in prehospital care stems primarily from a lack of confidence and familiarity with ventilation technology. He attributes this to inadequate initial training and continuing education. In his opinion, common training challenges (
Mechanical ventilators have long been perceived as complex, difficult to train staff on, and challenging to operate under pressure. Dr. Rugna disagrees. “Today’s machines are easy to learn and simple to use. The EMS staff only needs to input the patient group, height, and sex,” he explains.
He emphasizes that the user-friendly interfaces on today’s transport ventilators help ease the training burden on his team, making broader adoption of mechanical ventilation more feasible.

In addition, many ventilation technology providers are improving the services, training, and support resources they include with purchase of their devices. Solutions can incorporate flexible online training and certification programs, as well as software update services, preventive maintenance, and loaner device programs to minimize fleet downtime.


Along with improving technical training, Dr. Rugna suggests that prehospital providers incorporate stronger messaging around the impact of mechanical ventilation in the overall emergency care environment. He has seen dramatic changes in team dynamics and had success developing his practitioners by highlighting these “hidden” benefits at every stage of prehospital care.
“Starting mechanical airway support as quickly as possible calms the chaos of the emergency scene,” he explains, describing how the ventilator offers his team peace of mind while also freeing up their hands to focus on other interventions. As care continues during transport, the team dynamics shift, and treatment moves from constant activity to providing adjustments as needed. By the time the patient arrives at the hospital, treatment data is readily available, enabling a confident handoff and continuity of care.
Alleviating cognitive burdens for EMS providers (

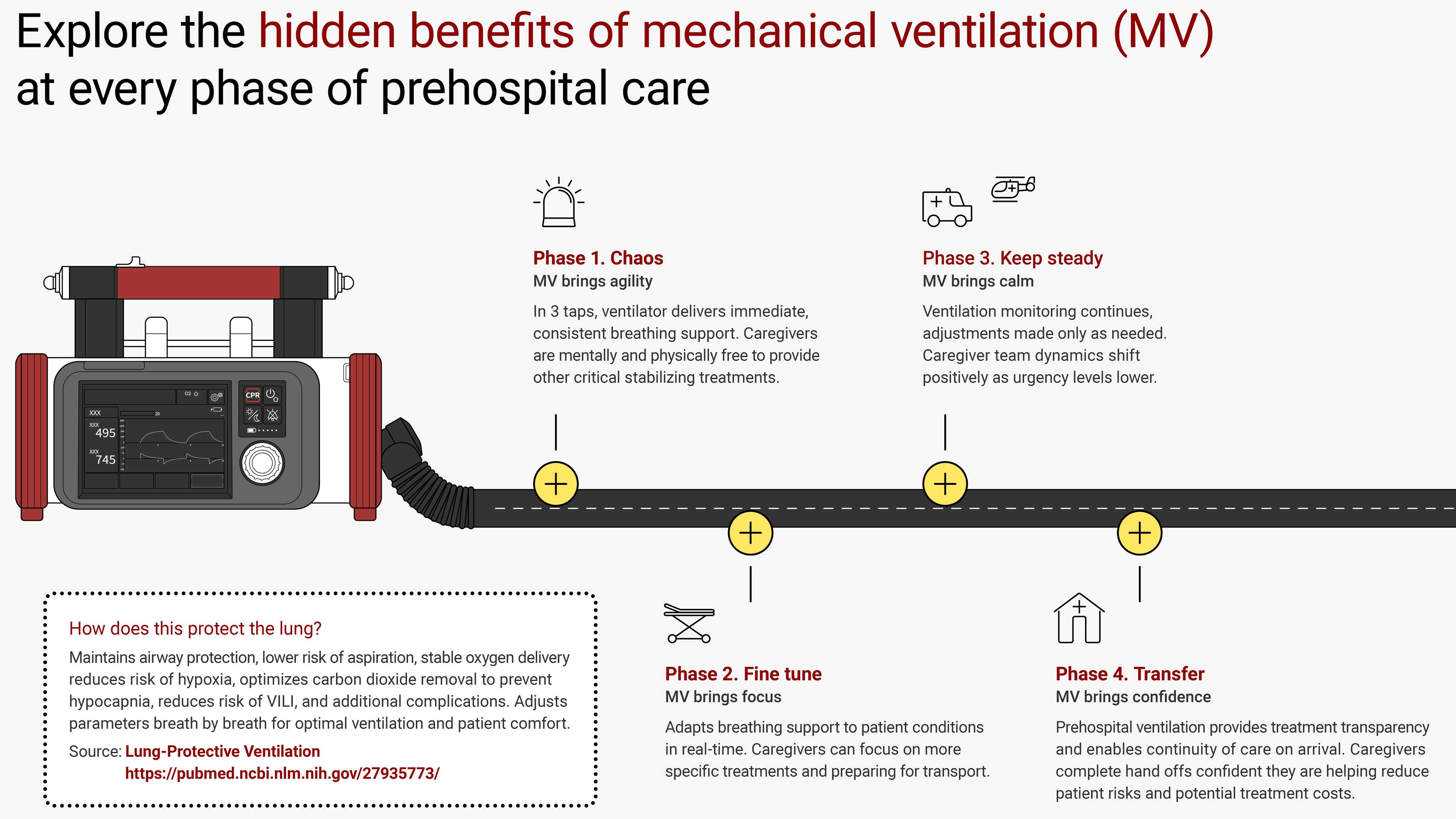
This new-found confidence brought on by mechanical ventilation extends across every stage of prehospital care.
The graphic above (
As prehospital technology advances, devices are becoming increasingly intelligent, interconnected, and capable of real-time clinical decision making.
Dr. Rugna envisions a future where a single device could deliver mechanical ventilation that is synchronized with chest compressions, to be used specifically in cardiac arrest emergencies. These innovations are already on the horizon, powered by developments in AI, waveform analytics, engineering, and cultural shifts toward greater connectivity.

Several other emerging technologies could also shape the next generation of prehospital ventilation and emergency care:

Modernizing training. Enhancing teamwork. Building confidence. This is how practitioners like Dr. Rugna envision the future of prehospital ventilation. He encourages prehospital leaders to focus their education on the hidden benefits of mechanical ventilation, confident that improvements in patient care will follow automatically.
By incorporating mechanical ventilation into their work, EMS teams can provide more comprehensive clinical treatment, enhance stabilization efforts, and strengthen the connection between prehospital and in-hospital care.
As transport ventilators continue to evolve in terms of both capability and portability, and with many intelligent, easy-to-use systems already available, the opportunity is clear: Equip EMS teams with the tools and support they need, and they will be empowered to deliver the right therapy at the right time, from the very first moment of care.
