Мы всегда готовы помочь и свяжемся с вами как можно скорее.

Наша глобальная команда и местные эксперты готовы оказать вам поддержку.

Получите доступ ко всем документам, видео, статьям, модулям дистанционного обучения и дополнительным ресурсам, связанным со всеми нашими продуктами.

Измерение пищеводного давления (Pes) — это малоинвазивный метод мониторинга, который позволяет определить транспульмональное давление.
Наиболее распространенный способ измерения значения Pes — с помощью наполненного воздухом баллона, встроенного в пищеводный катетер.
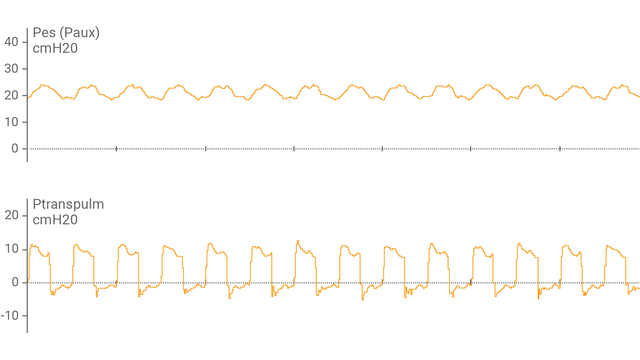
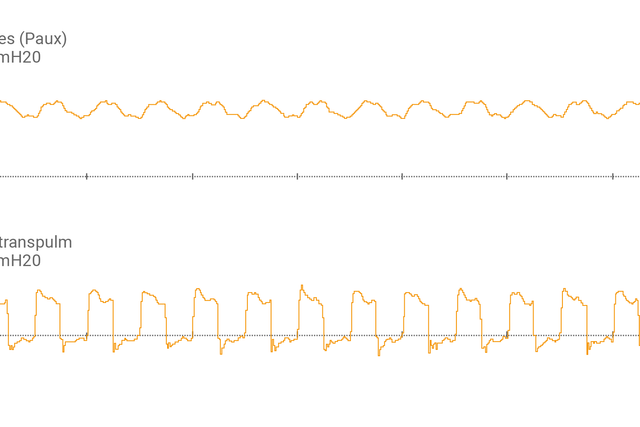
После подсоединения пищеводного баллонного катетера к вспомогательному порту и подтверждения правильности размещения на экране аппарата ИВЛ в виде кривой отобразится пищеводное давление (Pes) и транспульмональное давление (Ptranspulm).
Измерить статическое значение Ptranspulm можно с помощью маневров задержки вдоха и выдоха.

Для оценки возможности раскрытия объема легких и выполнения маневров рекрутмента также можно использовать транспульмональное давление в сочетании с инструментом P/V Tool® Pro.
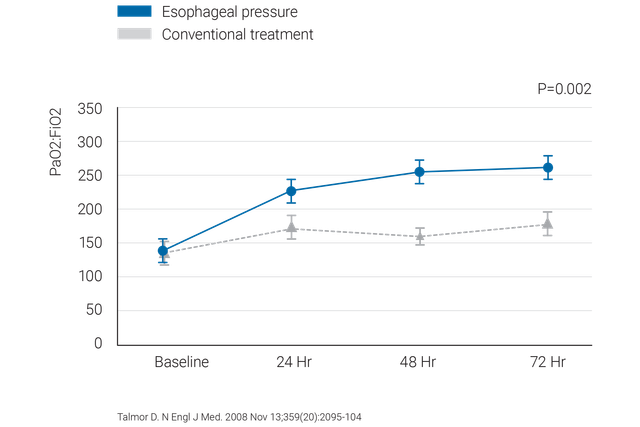

Посмотрите этот короткий ролик, чтобы узнать, как использовать мониторинг транспульмонального давления для более точной установки значения PEEP.


Клинически проверенные рекомендации касательно того, что следует делать и чего следует избегать при измерении пищеводного давления у пациентов с острым респираторным дистресс-синдромом.
Компания Hamilton Medical предлагает пищеводные баллонные катетеры производства компании Cooper Surgical и назогастральные катетеры производства компании NutriVent.
Мониторинг транспульмонального давления – это стандартная функция в аппаратах ИВЛ HAMILTON-C6 и HAMILTON-G5/S1.