



Autor: Jean-Michel Arnal, Hôpital Sainte Musse, Toulon, Frankreich
Datum: 18.09.2025
Last change: 10.06.2026
Typo correctionDer statische Driving Pressure sollte am Patientenbett systematisch überwacht werden, aber wie ermitteln wir ihn?
Bei maschinell mit assistierten Modi beatmeten Patienten ist der statische Driving Pressure (∆Pstat) unabhängig von anderen Werten mit dem Überleben eines Intensivstation-Aufenthaltes assoziiert (
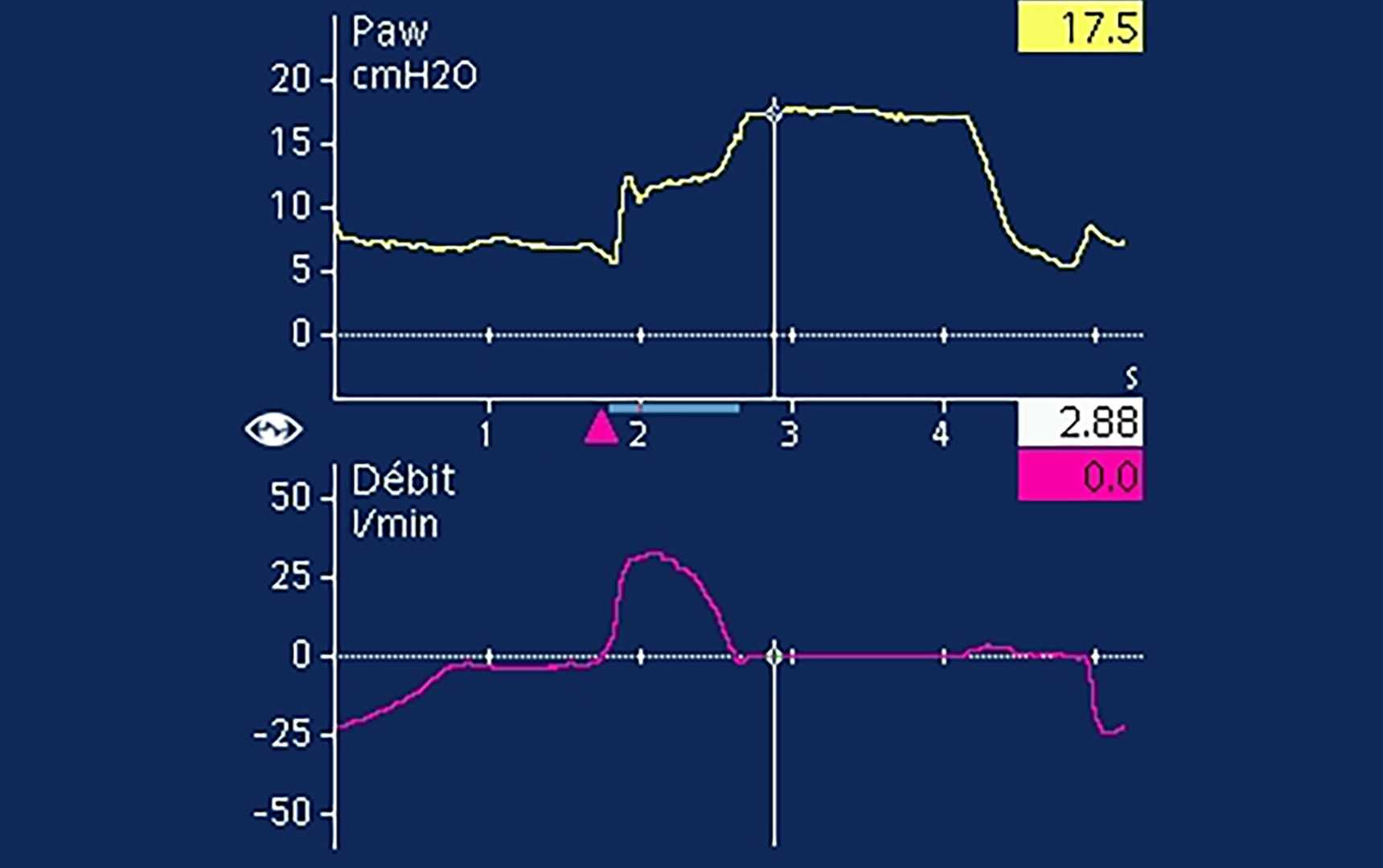
Eine endinspiratorische Okklusion dient zur Messung von Pplat in assistierten Atemhüben (

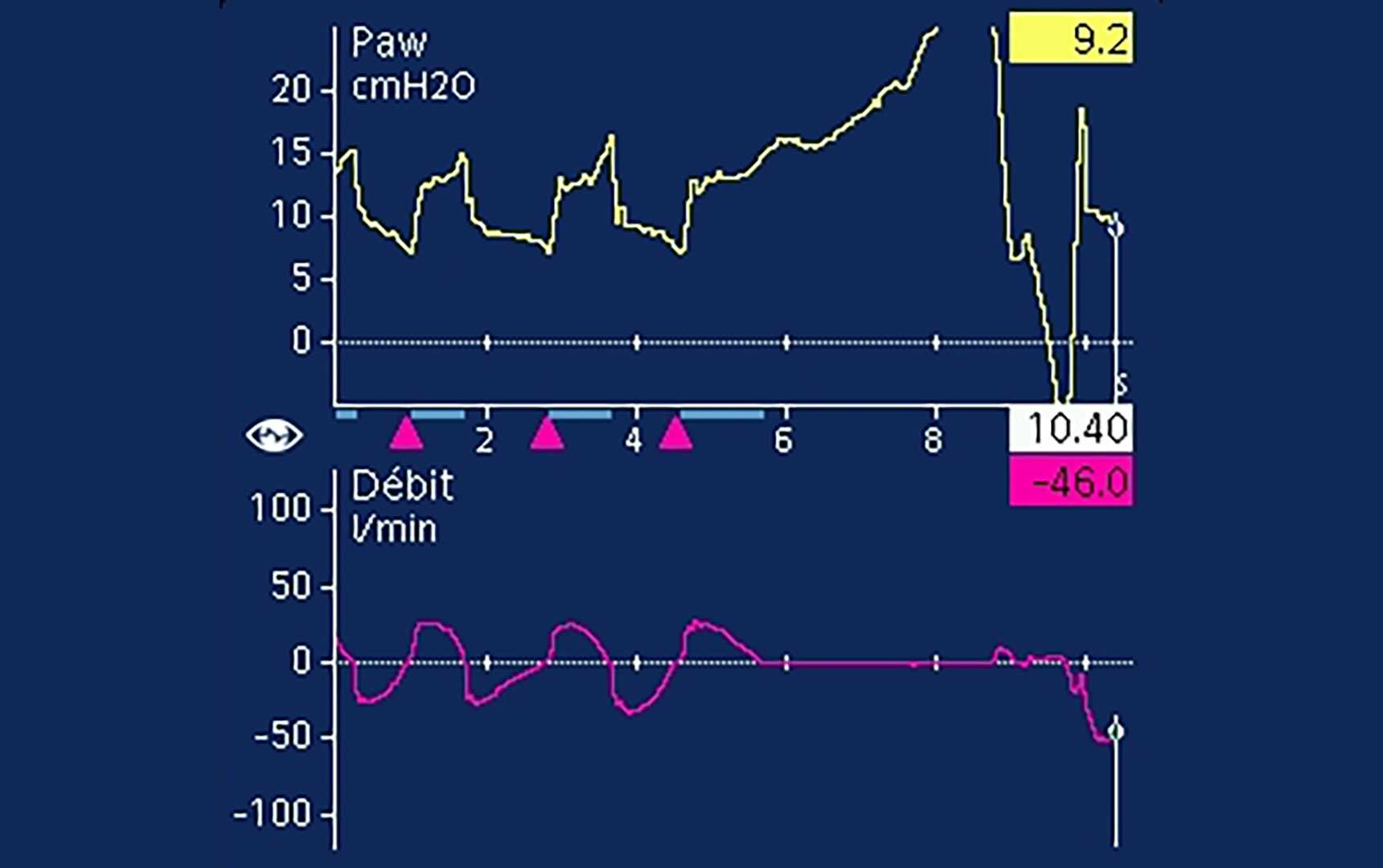

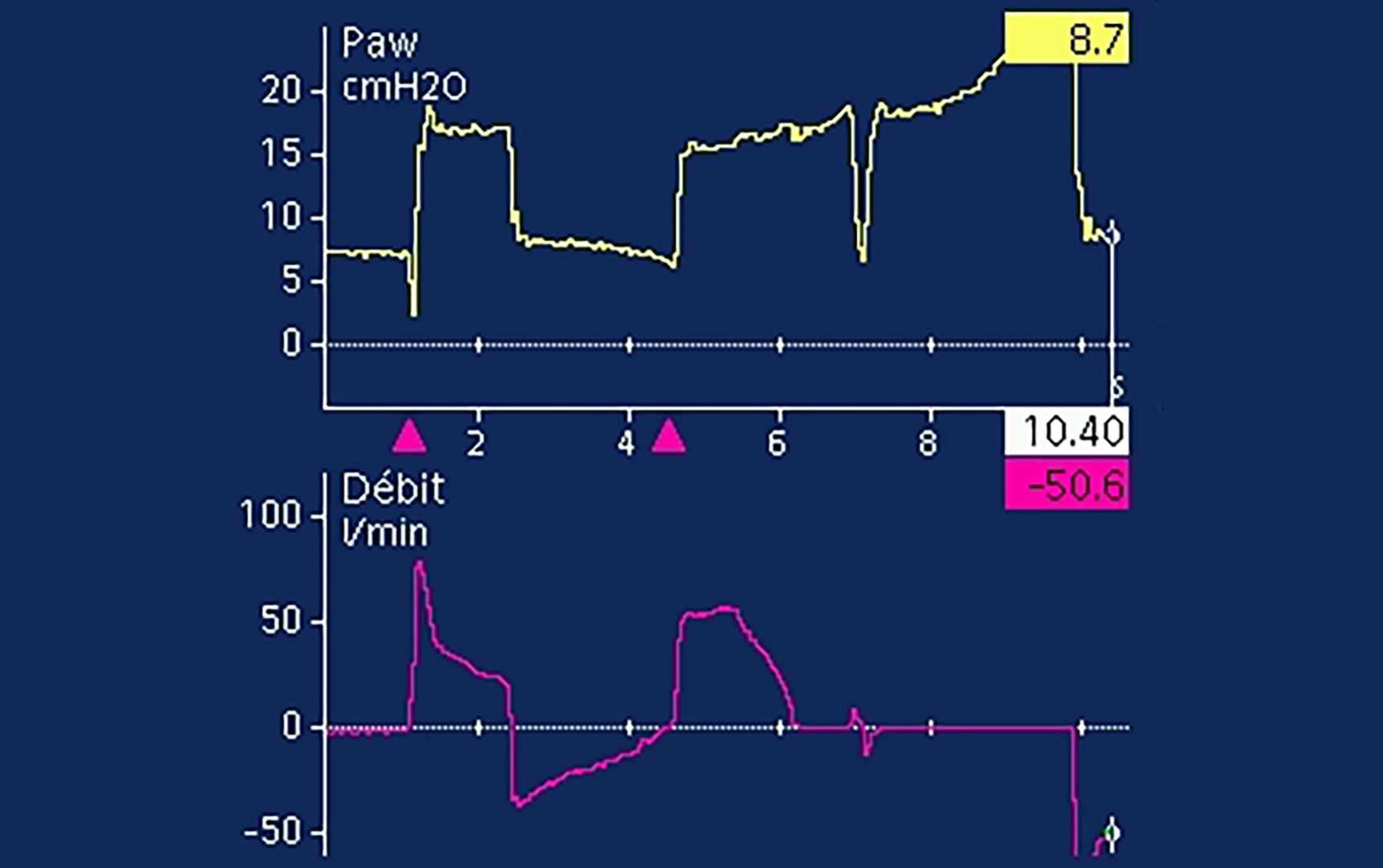
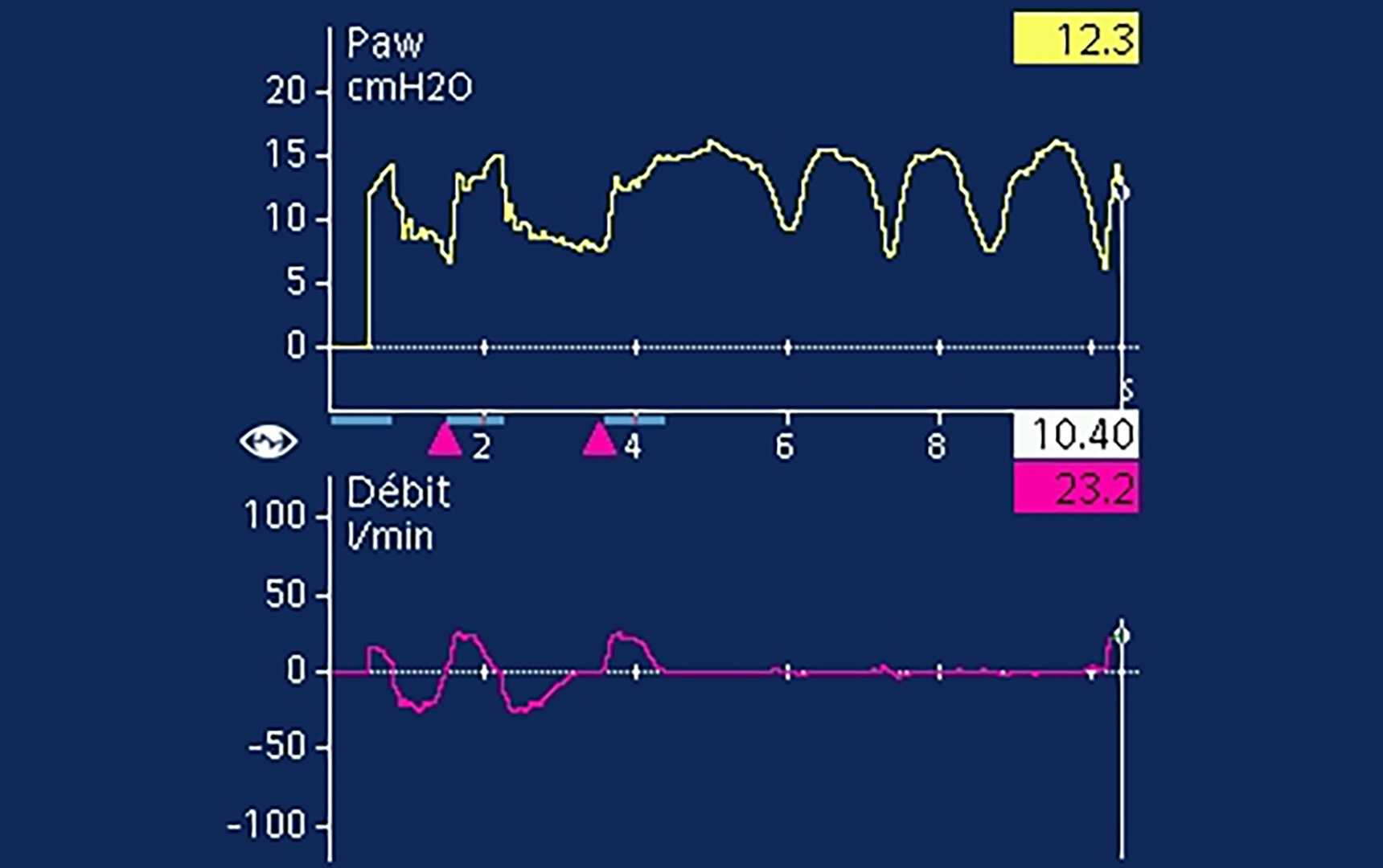
Selbst wenn ein klares Plateau sichtbar ist, liegt häufig eine Aktivität der exspiratorischen Muskeln vor (
